

Differential Effects of Ticagrelor With or Without Aspirin on Platelet Reactivity and Coagulation Activation: A Randomized Trial in Healthy Volunteers
- PMID: 31442298
- PMCID: PMC7006887
- DOI: 10.1002/cpt.1616
Differential Effects of Ticagrelor With or Without Aspirin on Platelet Reactivity and Coagulation Activation: A Randomized Trial in Healthy Volunteers
Abstract
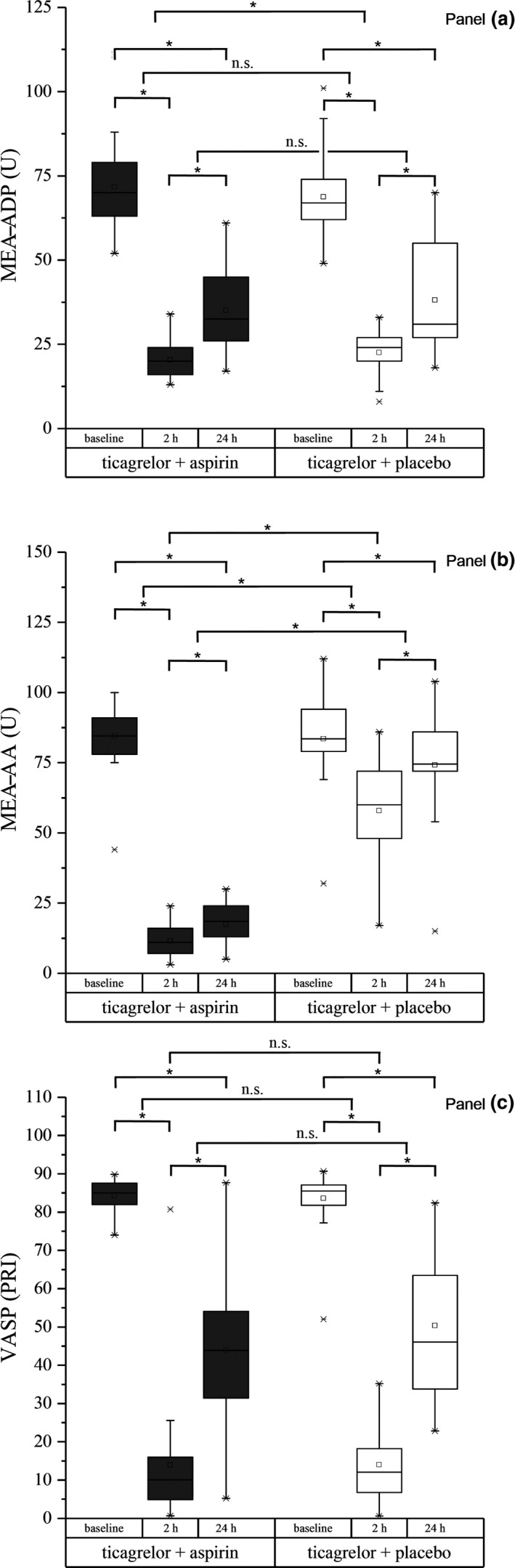
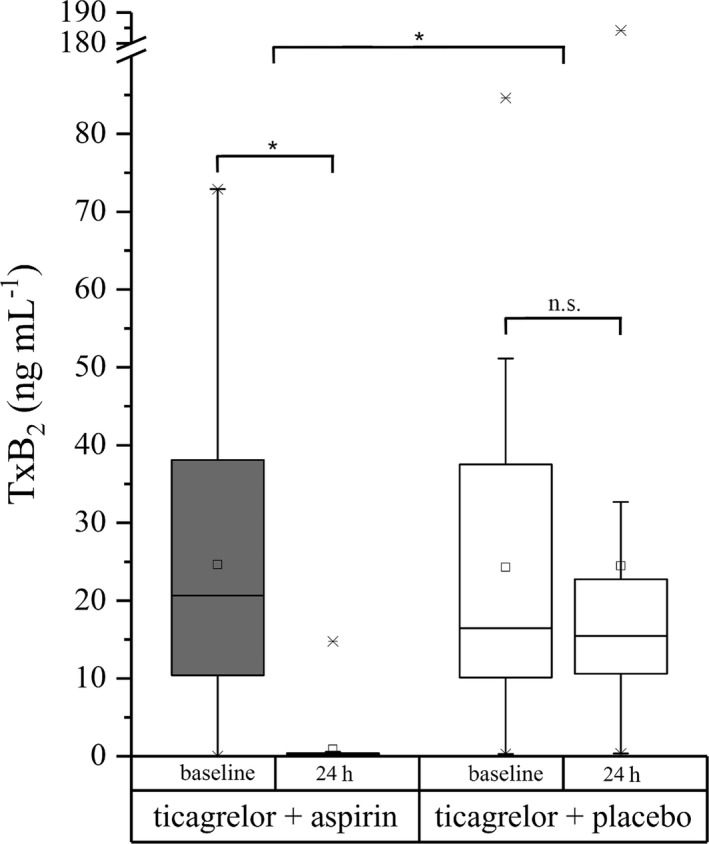
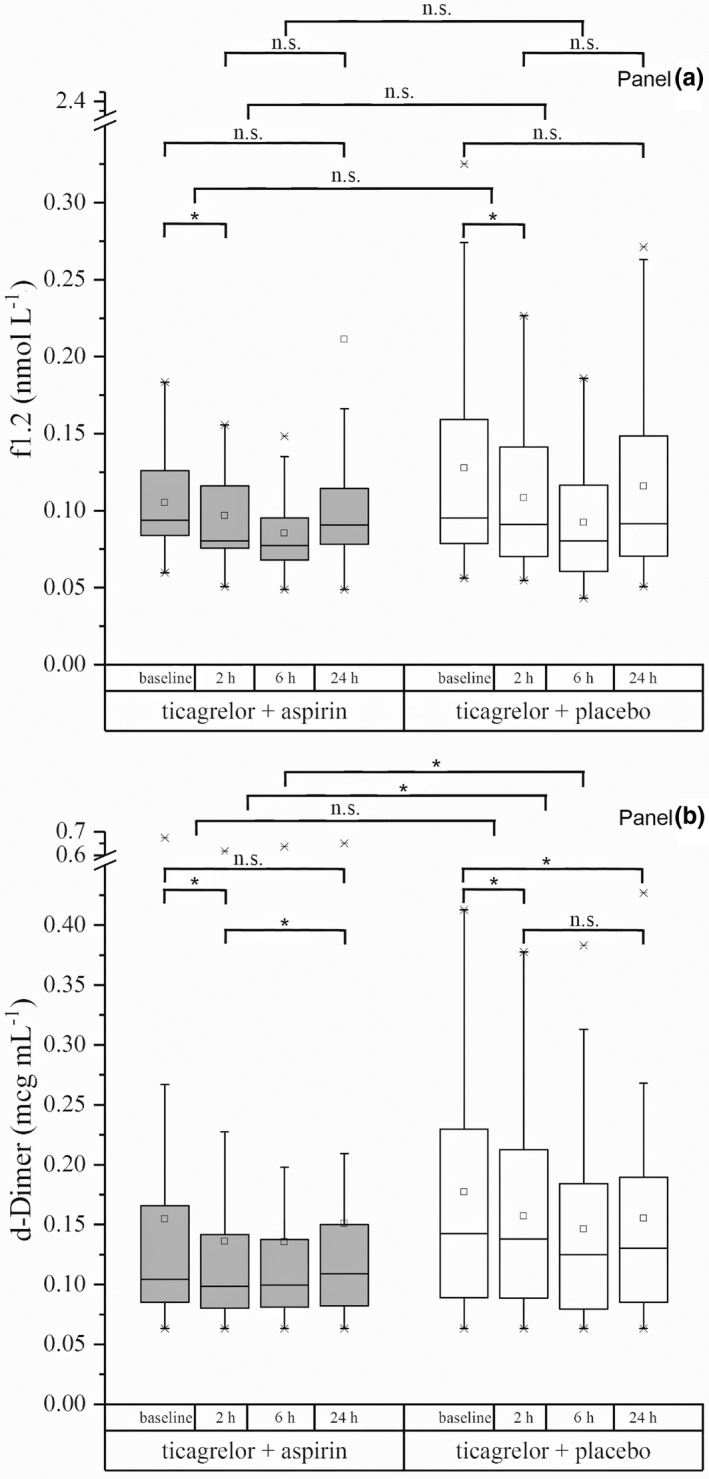
Dual antiplatelet therapy (DAPT) is standard in acute coronary heart disease but confers a bleeding risk. To compare the effects of ticagrelor-monotherapy with ticagrelor-based DAPT on hemostatic system activation, we conducted a randomized controlled trial in 44 volunteers using a loading-dose regimen and measured platelet-aggregometry triggered by adenosine diphosphate (multiple electrode aggregometry (MEA)-ADP) and arachidonic acid (MEA-AA), the vasodilator-stimulated phosphoprotein (VASP), prothrombin fragment 1.2 (f1.2), and d-Dimer. Ticagrelor-based DAPT and ticagrelor-monotherapy significantly decreased MEA-ADP (Δmean: -51.4 (-56.9; -45.8) and -46.2 (-51.7; -40.7)) and VASP (Δmean: -70.3 (-76.2; -64.4) and -69.6 (-75.5; -63.7)) at 2 hours and over 24 hours. MEA-AA was reduced significantly by both treatments (Δmean: -72.9 (-80.6; -65.3) and -25.7 (-33.3; -18.0)) at 2 hours, and stronger by ticagrelor-based DAPT over 24 hours. Both treatments decreased f1.2 (geometric mean ratio (GMR): 0.92 (0.84; 1.01) and 0.88 (0.80; 0.96)) and d-Dimer (GMR: 0.89 (0.86; 0.92) and 0.91 (0.88; 0.94)) at 2 hours and d-Dimer over 24 hours. Ticagrelor-monotherapy and ticagrelor-based DAPT comparably affect hemostatic system activation.
© 2019 The Authors. Clinical Pharmacology & Therapeutics published by Wiley Periodicals, Inc. on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
Jolanta M. Siller‐Matula reports lecture or consultant fees from Bayer, Astra Zeneca, Eli Lilly, Daiichi‐Sankyo, and Roche. All other authors declared no competing interests for this work.
Figures
References
-
- Nichols, M. , Townsend, N. , Scarborough, P. & Rayner, M. Cardiovascular disease in Europe 2014: epidemiological update. Eur. Heart J. 35, 2950–2959 (2014). - PubMed
-
- Alpert, J.S. , Thygesen, K. , Antman, E. & Bassand, J.P. Myocardial infarction redefined – a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J. Am. Coll. Cardiol. 36, 959–969 (2000). - PubMed
-
- Reed, G.W. , Rossi, J.E. & Cannon, C.P. Acute myocardial infarction. Lancet 389, 197–210 (2016). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
