

Acute kidney injury from sepsis: current concepts, epidemiology, pathophysiology, prevention and treatment
- PMID: 31443997
- PMCID: PMC6920048
- DOI: 10.1016/j.kint.2019.05.026
Acute kidney injury from sepsis: current concepts, epidemiology, pathophysiology, prevention and treatment
Abstract
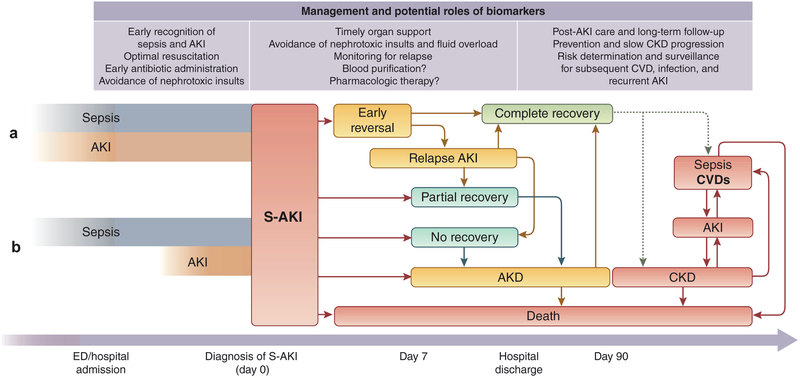
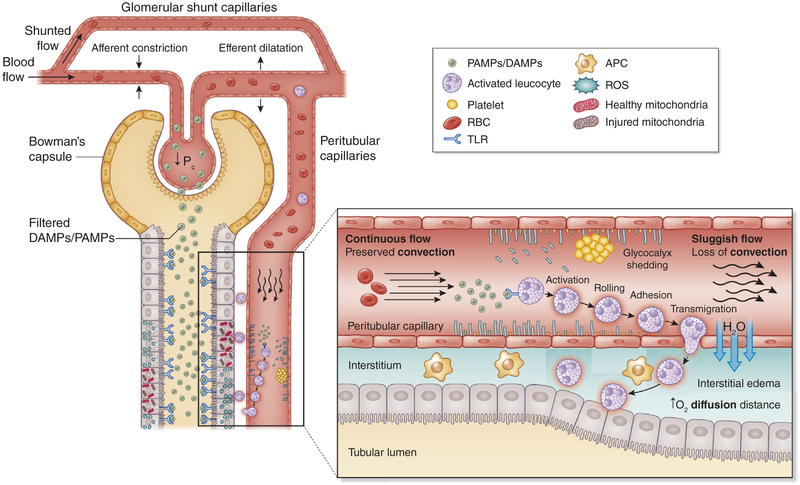
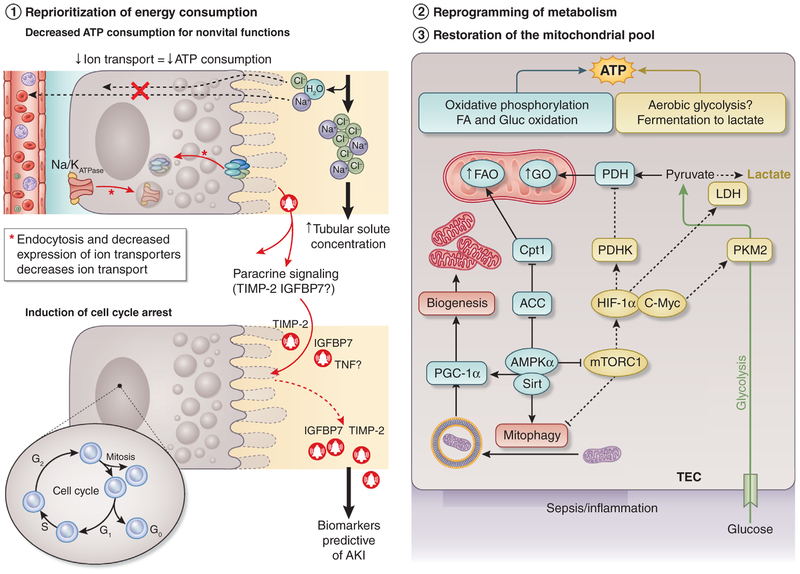
Sepsis-associated acute kidney injury (S-AKI) is a frequent complication of the critically ill patient and is associated with unacceptable morbidity and mortality. Prevention of S-AKI is difficult because by the time patients seek medical attention, most have already developed acute kidney injury. Thus, early recognition is crucial to provide supportive treatment and limit further insults. Current diagnostic criteria for acute kidney injury has limited early detection; however, novel biomarkers of kidney stress and damage have been recently validated for risk prediction and early diagnosis of acute kidney injury in the setting of sepsis. Recent evidence shows that microvascular dysfunction, inflammation, and metabolic reprogramming are 3 fundamental mechanisms that may play a role in the development of S-AKI. However, more mechanistic studies are needed to better understand the convoluted pathophysiology of S-AKI and to translate these findings into potential treatment strategies and add to the promising pharmacologic approaches being developed and tested in clinical trials.
Keywords: epidemiology; inflammation; metabolic reprogramming; microvascular dysfunction; prevention; sepsis-associated acute kidney injury; sepsis-induced acute kidney injury; treatment.
Copyright © 2019 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
DISCLOSURE
JAK discloses grant support and consulting fees from Astute Medical, Baxter, bioMerieux, BioPorto, and NxStage. All the other authors declared no competing interests.
Figures
References
-
- Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. - PubMed
-
- Bagshaw SM, Uchino S, Bellomo R, et al. Septic acute kidney injury in critically ill patients: clinical characteristics and outcomes. Clin J Am Soc Nephrol. 2007;2:431–439. - PubMed
-
- Hoste EA, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41:1411–1423. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
