

Subcutaneous concizumab prophylaxis in hemophilia A and hemophilia A/B with inhibitors: phase 2 trial results
- PMID: 31444162
- PMCID: PMC6895373
- DOI: 10.1182/blood.2019001542
Subcutaneous concizumab prophylaxis in hemophilia A and hemophilia A/B with inhibitors: phase 2 trial results
Abstract
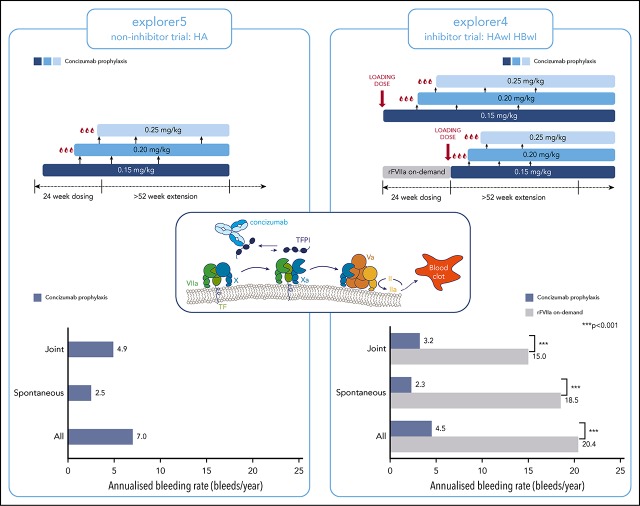
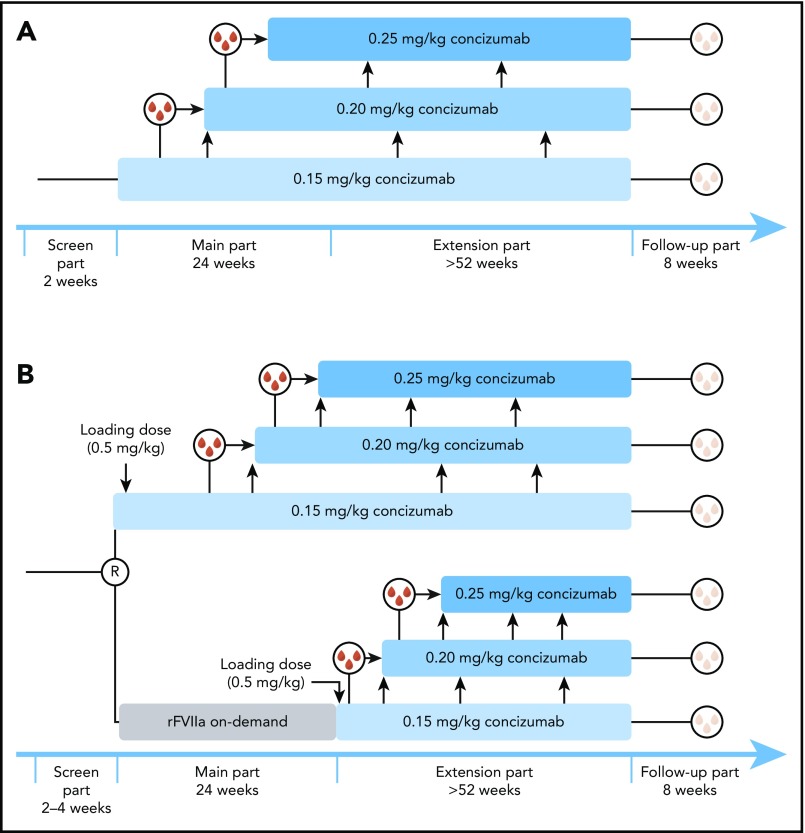
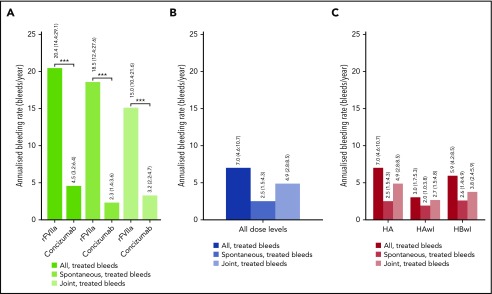
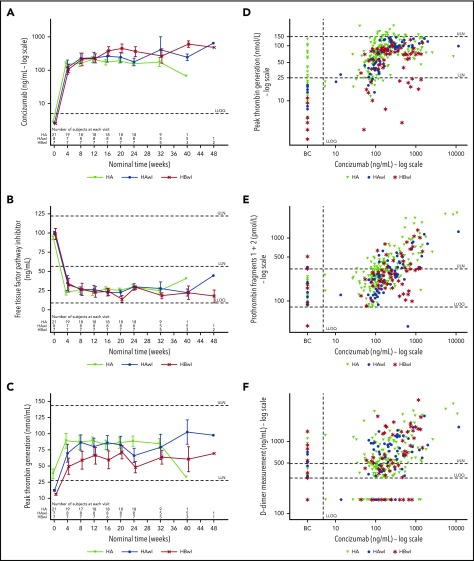
Results from the main parts (24 weeks) of 2 concizumab phase 2 trials are presented: explorer4 in hemophilia A (HA) or B (HB) with inhibitors (HAwI/HBwI) and explorer5 in HA. The trials aimed to evaluate the efficacy of daily subcutaneous concizumab prophylaxis (evaluated as annualized bleeding rate [ABR] at last dose level), with secondary objectives being safety and immunogenicity (assessed as number of adverse events [AEs] and antidrug antibodies [ADAs]). Patients received 0.15 mg/kg concizumab, with potential dose escalation to 0.20 and 0.25 mg/kg (if ≥3 spontaneous bleeding episodes within 12 weeks of concizumab treatment). Relevant pharmacokinetic/pharmacodynamic (PK/PD) parameters were assessed. Thirty-six HA, 9 HAwI, and 8 HBwI patients were exposed to concizumab. Most inhibitor patients (15 of 17; 88.2%) did not escalate the dose; all patients chose to continue to the extension phase of the trials. Clinical proof of concept for prevention of bleeding episodes was demonstrated in both trials. Estimated ABRs in HAwI and HBwI were lower vs HA: 3.0 (95% confidence interval [CI], 1.7; 5.3) and 5.9 (95% CI, 4.2; 8.5) vs 7.0 (95% CI, 4.6; 10.7), respectively. PK/PD results were as expected, with no difference between hemophilia subtypes for concizumab exposure, free tissue factor pathway inhibitor, thrombin generation, prothrombin fragment 1+2, and d-dimers. Concizumab was safe and well tolerated (no severe AEs, AE-related withdrawals, or thromboembolic events). Three patients had (very low to medium titer) ADA+ tests in each trial, with no observed clinical effect. These results support further development of concizumab as a daily prophylactic treatment in all hemophilia patients. These trials were registered at www.clinicaltrials.gov as #NCT03196284 and #NCT03196297.
© 2019 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: A.D.S. serves as principal investigator on 3 Novo Nordisk–sponsored research studies. J.A. has received honoraria and consulting fees from Bayer, CSL Behring, Novo Nordisk, Octapharma, Roche, Sobi, Spark, Takeda, and uniQure. G.B. has received grants and personal fees for lectures and consultancy from Bayer, Boehringer Ingelheim, CSL Behring, Novo Nordisk, Pfizer, Shire, and Sobi. G.C. participated in a uniQure advisory board meeting; received fees to act as a speaker from, or to participate in advisory board meetings for, Ablynx, Bayer, CSL Behring, Kedrion, Novo Nordisk, Shire/Takeda, Sobi, Roche, and Werfen; and received research grants from CSL Behring, Pfizer, and Sobi. P.C. has received honoraria from Baxalta/Shire, Biogen Idec, CSL Behring, Novo Nordisk, Pfizer, Roche and Sobi; has served on advisory boards for Bayer, Baxalta/Shire, Biogen Idec, CSL Behring, Chugai, Freeline, Novo Nordisk, Pfizer, Roche, and Sobi; and has received research funding from Bayer, CSL Behring, Novo Nordisk, Pfizer, and Sobi. H.E. has received fees to act as a speaker or consultant from, or to participate in advisory board meetings for, Bayer, CSL Behring, Novo Nordisk, Shire/Takeda, Sobi, and Roche, and has received research grants from Bayer Vital, CSL Behring, and Pfizer. V.J.-Y. has received reimbursement for attending symposia/congresses and/or honoraria for speaking and/or consulting and/or funds for research from Bayer, CSL Behring, Grifols, Novo Nordisk, Octapharma, Pfizer, Roche, Sobi, and Shire. K.K. has participated in advisory board meetings for Bayer, Novo Nordisk, Takeda, Pfizer, and Roche. T.M. has received honoraria from Bayer, Bioverative, Chugai, CSL, KM Biologics, Novo Nordisk, and Shire, and research support from Bayer and Bioverative. L.H.P. has received funding for attending congresses and meetings from Bayer, Novo Nordisk, Pfizer, and Sobi. A.P.W. has participated in advisory board meetings for Biomarin, Novo Nordisk, Octapharma, Shire, and uniQure. G.Y. has received honoraria and consulting fees from Bioverativ/Sanofi, CSL Behring, Genentech/Roche, Grifols, Kedrion, Novo Nordisk, Spark, Takeda, and uniQure. S.Z.-S. has received reimbursement for attending symposia and congresses, and honoraria payment for speaking, from Biogen, Novo Nordisk, Sobi, and Roche. J.O. has received reimbursement for attending symposia/congresses and/or honoraria for speaking and/or consulting and/or funds for research from Bayer, Biogen Idec, Biotest, Chugai, CSL Behring, Grifols, Novo Nordisk, Octapharma, Pfizer, Roche, Taked, and Swedish Orphan Biovitrum. P.A. declares no competing financial interests.
Figures
Comment in
-
TFPI blockade: removing coagulation's brakes.Blood. 2019 Nov 28;134(22):1885-1887. doi: 10.1182/blood.2019002900. Blood. 2019. PMID: 31778542 No abstract available.
References
-
- Bolton-Maggs PH, Pasi KJ. Haemophilias A and B. Lancet. 2003;361(9371):1801-1809. - PubMed
-
- Srivastava A, Brewer AK, Mauser-Bunschoten EP, et al. . Guidelines for the management of hemophilia. Haemophilia. 2013;19(1):e1-e47. - PubMed
-
- Hacker MR, Geraghty S, Manco-Johnson M. Barriers to compliance with prophylaxis therapy in haemophilia. Haemophilia. 2001;7(4):392-396. - PubMed
-
- Petrini P. Identifying and overcoming barriers to prophylaxis in the management of haemophilia. Haemophilia. 2007;13(suppl 2):16-22. - PubMed
-
- Santagostino E, Mancuso ME. Venous access in haemophilic children: choice and management. Haemophilia. 2010;16(suppl 1):20-24. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
