

Glomerular Immunodeposits of Patients with IgA Nephropathy Are Enriched for IgG Autoantibodies Specific for Galactose-Deficient IgA1
- PMID: 31444275
- PMCID: PMC6779349
- DOI: 10.1681/ASN.2018111156
Glomerular Immunodeposits of Patients with IgA Nephropathy Are Enriched for IgG Autoantibodies Specific for Galactose-Deficient IgA1
Abstract
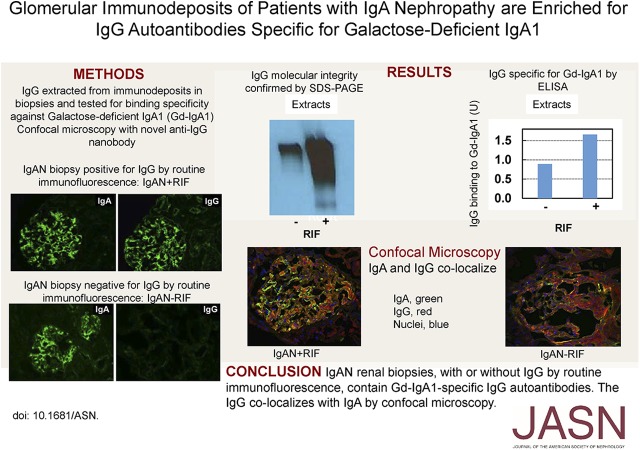
Background: IgA nephropathy (IgAN) is the leading primary GN worldwide. The disease is thought to result from glomerular deposition of circulating immune complexes of IgG bound to galactose-deficient IgA1 (Gd-IgA1). However, routine immunofluorescence microscopy fails to detect IgG in many kidney biopsies from patients with IgAN and the specificity of IgG in immunodeposits has not been tested.
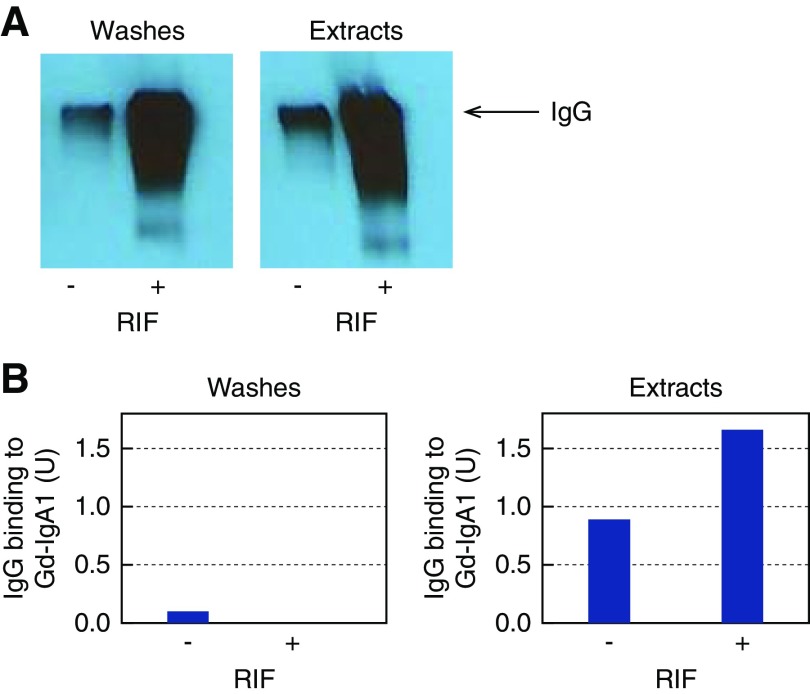
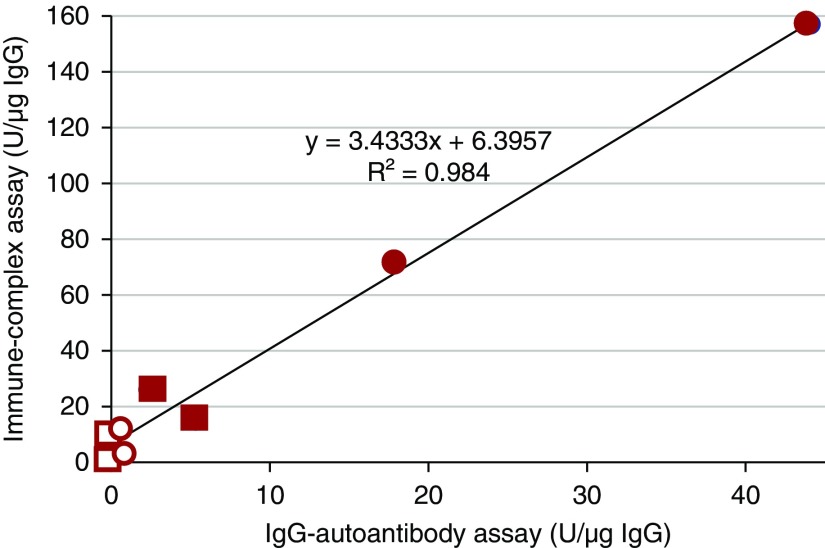
Methods: We used remnant frozen kidney-biopsy specimens from 34 patients with IgAN; 14 were IgG-positive and 20 were IgG-negative by routine immunofluorescence microscopy. Six patients with primary membranous nephropathy (MN) and eight with lupus nephritis (LN) served as controls. IgG in the kidney tissue was extracted and its amount determined by ELISA. IgG molecular integrity was assessed by SDS-PAGE immunoblotting. Antigenic specificity of extracted IgG was determined by ELISA using phospholipase A2 receptor (PLA2R) or Gd-IgA1 as antigen. In addition, ten other IgAN cases, six IgG-positive and four IgG-negative by routine immunofluorescence, were used for colocalization studies by confocal microscopy.
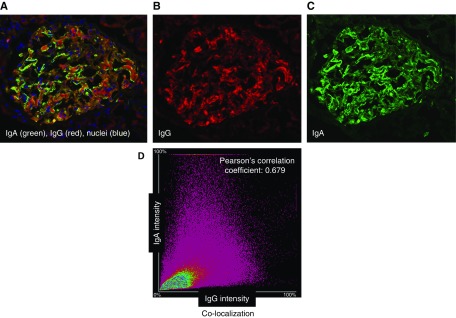
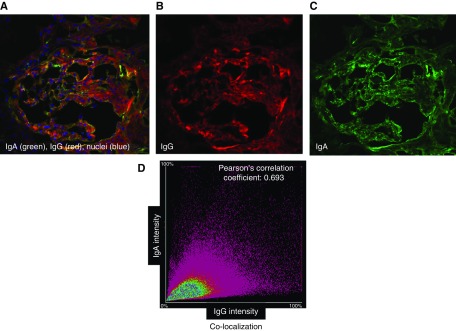
Results: IgG extracted from MN but not IgAN immunodeposits reacted with PLA2R. Conversely, IgG extracted from IgAN but not MN or LN immunodeposits reacted with Gd-IgA1. Even IgAN kidney-biopsy specimens without IgG by routine immunofluorescence microscopy had IgG specific for Gd-IgA1. Confocal microscopy confirmed the presence of IgG in the IgAN biopsies with colocalization of glomerular IgA and IgG.
Conclusions: These results reveal for the first time that IgAN kidney biopsies, with or without IgG by routine immunofluorescence, contain Gd-IgA1-specific IgG autoantibodies. These findings support the importance of these autoantibodies in the pathogenesis of IgAN.
Keywords: IgA nephropathy; autoantibody; biomarker; immunodeposits.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Wyatt RJ, Julian BA: IgA nephropathy. N Engl J Med 368: 2402–2414, 2013 - PubMed
-
- Hiki Y, Odani H, Takahashi M, Yasuda Y, Nishimoto A, Iwase H, et al. .: Mass spectrometry proves under-O-glycosylation of glomerular IgA1 in IgA nephropathy. Kidney Int 59: 1077–1085, 2001 - PubMed
-
- Allen AC, Bailey EM, Brenchley PE, Buck KS, Barratt J, Feehally J: Mesangial IgA1 in IgA nephropathy exhibits aberrant O-glycosylation: Observations in three patients. Kidney Int 60: 969–973, 2001 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
