

Impact of Surgical Technique on Surgical Margin Status Following Partial Cystectomy
- PMID: 31445895
- PMCID: PMC7696003
- DOI: 10.1016/j.urolonc.2019.07.018
Impact of Surgical Technique on Surgical Margin Status Following Partial Cystectomy
Abstract
Introduction: We assessed the impact of open or minimally-invasive partial cystectomy on surgical margin status in a nationwide hospital-based cohort.
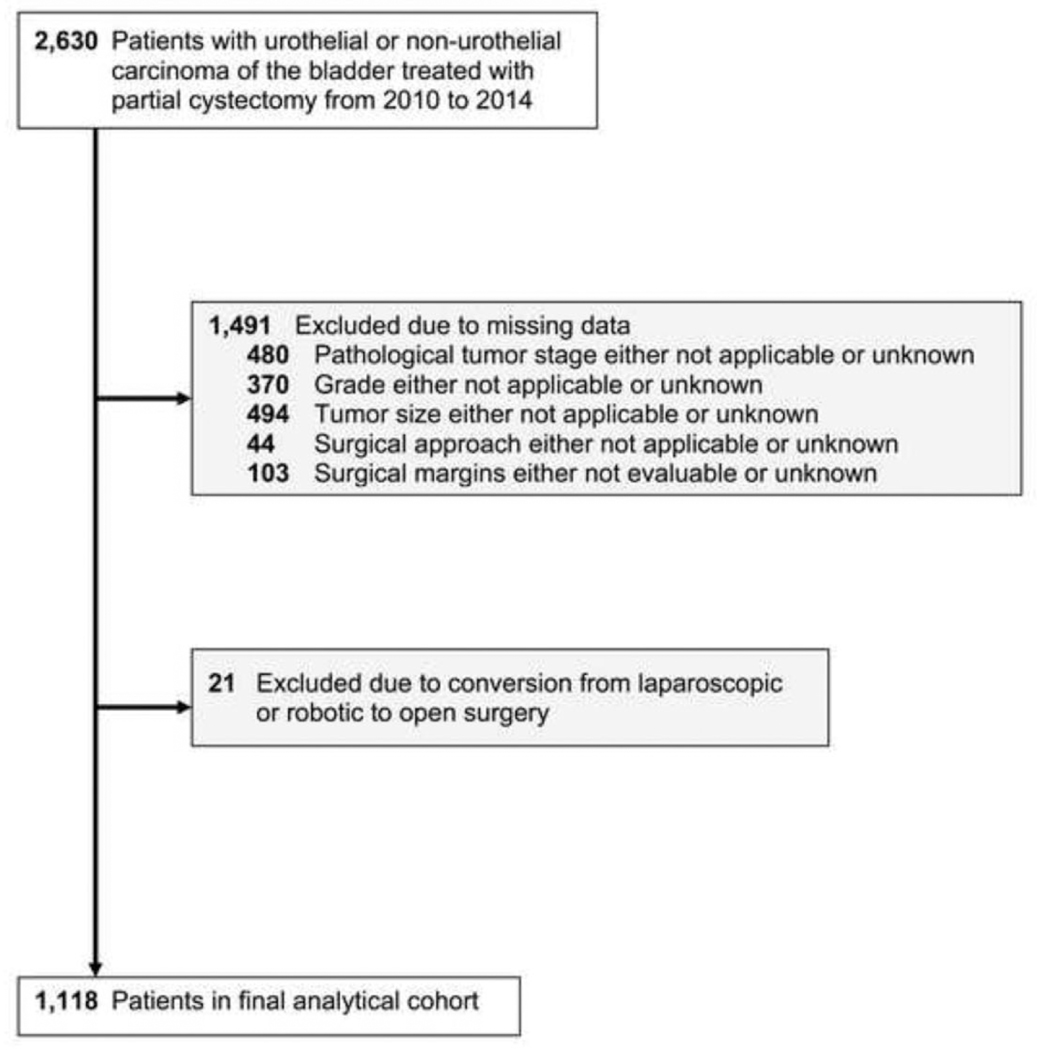
Materials and methods: Patients who underwent partial cystectomy from 2010 to 2014 were identified in the National Cancer Data Base. The primary outcome was surgical margin status. A multivariable logistic regression model was fitted to identify patient, hospital, and surgical factors associated with positive surgical margins (PSMs).
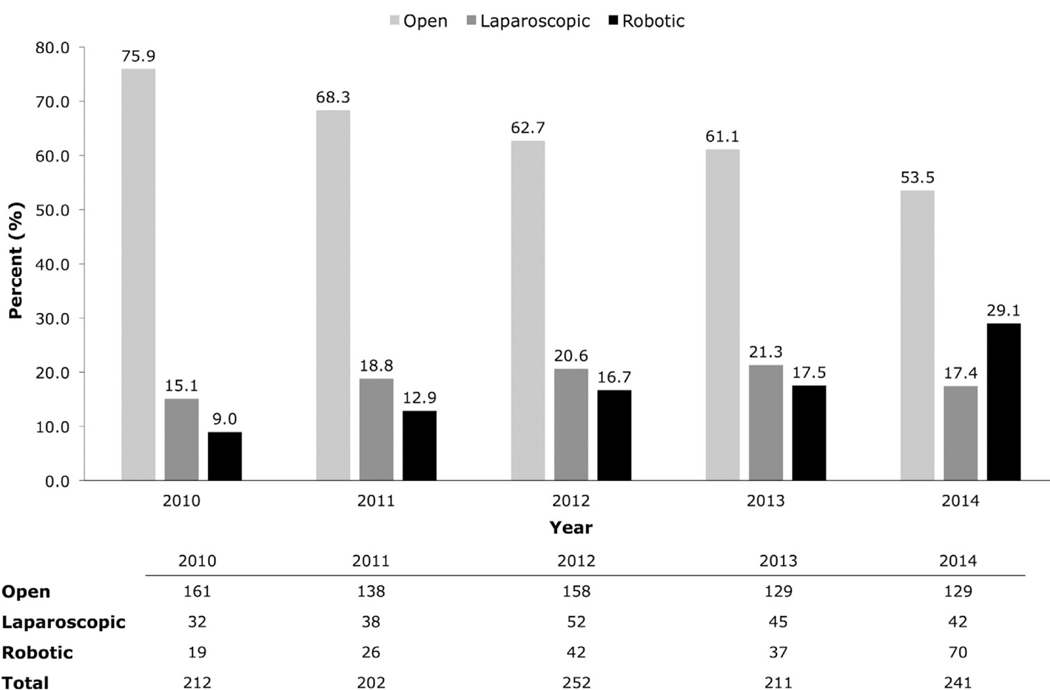
Results: Partial cystectomy was performed in 1,118 patients via open (n = 715, 64%), laparoscopic (n = 209, 19%), and robotic (n = 194, 17%) approaches. Overall, 220 (19.7%) patients had PSMs. The PSM rate by surgical approach was 19.6% for open, 18.2% for laparoscopic, and 21.6% for robotic (P = 0.678). Compared to open partial cystectomy, the laparoscopic (aOR 1.06, 95%CI 0.70-1.60, P = 0.782), and robotic (aOR 1.28, 95%CI 0.85-1.91, P = 0.235) approaches were not significantly different in terms of PSM rate. There were higher odds of PSMs in non-Hispanic blacks (aOR 1.93, 95%CI 1.09-3.39, P = 0.023) compared to non-Hispanic whites, and in patients with muscle invasive bladder cancer (aOR 3.28, 95%CI 2.00-5.37, P < 0.001) or tumor size ≥ 3 cm (aOR 1.67, 95%CI 1.21-2.30, P = 0.002). Tumors in a dome/urachal location had lower odds of a PSM compared to tumors in a nondome/urachal location (aOR 0.67, 95%CI 0.47-0.94, P = 0.022).
Conclusions: Our results suggest that partial cystectomy using a laparoscopic or robotic-assisted approach is not associated with an increased risk of PSMs compared to open partial cystectomy.
Keywords: Cystectomy; Margins of excision; Outcome and process assessment (health care); Urinary bladder neoplasm; Urologic surgical procedures.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018;68:7–30. - PubMed
-
- Hollenbeck BK, Taub DA, Dunn RL, Wei JT. Quality of care: partial cystectomy for bladder cancer—a case of inappropriate use? J Urol 2005;174: 1050–4; discussion 4. - PubMed
-
- NCC Network. Bladder cancer: NCCN Clinical Practice Guideline in Oncology (NCN GuidelineTM) Version 2.2017. National Comprehensive Cancer Network; 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
