

Combination denosumab and high dose teriparatide for postmenopausal osteoporosis (DATA-HD): a randomised, controlled phase 4 trial
- PMID: 31447409
- PMCID: PMC6980341
- DOI: 10.1016/S2213-8587(19)30255-4
Combination denosumab and high dose teriparatide for postmenopausal osteoporosis (DATA-HD): a randomised, controlled phase 4 trial
Abstract
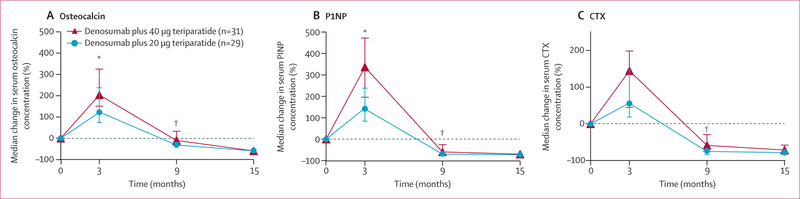
Background: In the Denosumab and Teriparatide Administration (DATA) study, we showed that denosumab fully inhibits teriparatide-induced bone resorption while allowing for continued teriparatide-induced bone formation, resulting in larger increases in hip and spine bone mineral density (BMD) than with either drug alone. We aimed to assess whether administration of denosumab with high dose teriparatide would stimulate larger increases in bone mass than those observed in the DATA study.
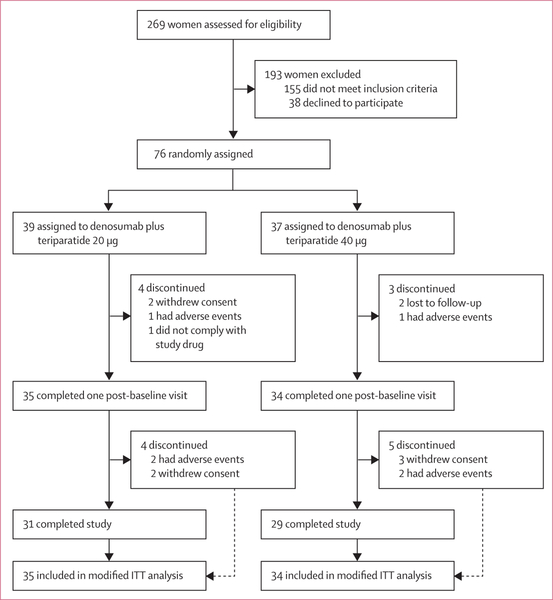
Methods: DATA-HD was an open-label, randomised, controlled phase 4 trial done at Massachusetts General Hospital. Eligible women were postmenopausal women (at least 36 months since last menses or since hysterectomy with a follicle-stimulating hormone concentration of ≥40 U/L) with osteoporosis. Participants were randomly assigned (1:1) to receive teriparatide 20 μg (standard dose) or 40 μg (high dose) daily via subcutaneous injection for 9 months. At 3 months, both groups were started on denosumab 60 mg every 6 months via subcutaneous injection for 12 months. Areal BMD (aBMD) was measured at 0, 3, 9, and 15 months. Treatment was given open label, but outcome assessors were masked. The primary endpoint was percentage change from baseline in spine areal BMD (aBMD) at 15 months. Women who completed at least one study visit after baseline were included in the modified intention-to-treat analysis. Safety was assessed in all randomly assigned participants. This study is registered with ClinicalTrials.gov, number NCT02176382.
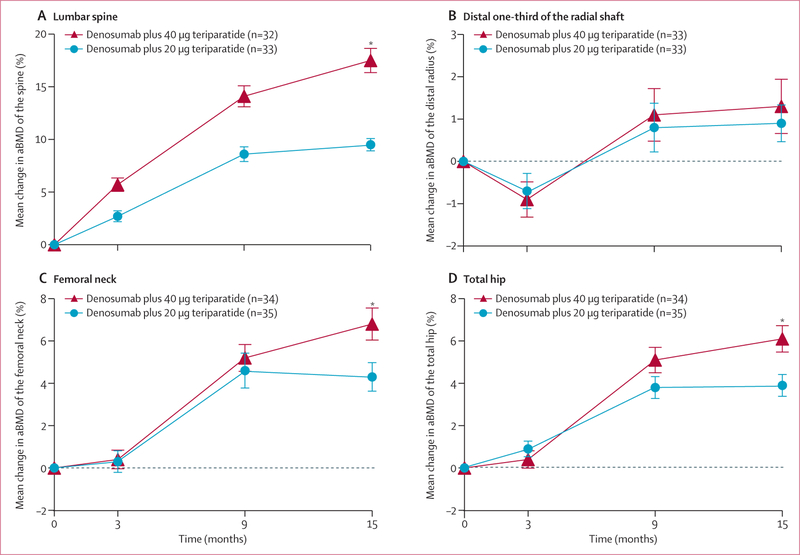
Findings: Between Oct 15, 2014, and June 10, 2016, 269 women were assessed for eligibility. 76 participants were randomly assigned to 20 μg teriparatide (n=39) or 40 μg teriparatide (n=37), of whom 69 completed at least one post-baseline visit. At 15 months, mean spine aBMD had increased to a significantly greater extent in the 40 μg group (17·5% [SD 6·0] increase) than the 20 μg group (9·5% [3·2]; difference 8·1%, 95% CI 5·5 to 10·6, p<0·0001). Mean femoral neck aBMD had also increased to a greater extent in the 40 μg group (6·8% [SD 4·1] increase) than the 20 μg group (4·3% [3·7]; difference 2·5%, 0·5 to 4·5, p=0·04), as did mean total hip aBMD (40 μg group, 6·1% [3·4] increase; 20 μg group, 3·9% [2·9] increase; difference 2·2%, 0·6 to 3·8, p<0·0001). 30 (77%) of 39 participants in the 20 μg group and 29 (78%) of 37 participants in the 40 μg group had an adverse event, and seven (18%) and two (5%) patients had serious adverse events. The most frequent adverse events were joint pain (15 [38%]), muscle cramp (15 [38%]), and fatigue (12 [31%]) in the 20 μg group group and fatigue (14 [38%]), nausea (16 [43%]), and joint pain (17 [46%]) in the 40 μg group. No deaths were reported.
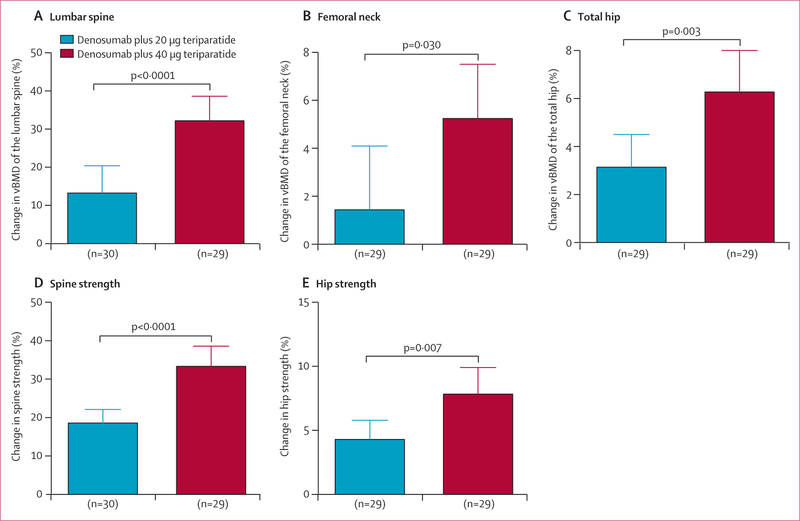
Interpretation: Combined treatment with teriparatide 40 μg and denosumab increases spine and hip BMD more than standard combination therapy. This large and rapid increase in bone mass suggest that this high dose regimen might provide a method of restoring skeletal integrity in patients with osteoporosis.
Funding: National Institutes of Health and the Dart Foundation.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Personalising osteoporosis treatment for patients at high risk of fracture.Lancet Diabetes Endocrinol. 2019 Oct;7(10):739-741. doi: 10.1016/S2213-8587(19)30266-9. Epub 2019 Aug 22. Lancet Diabetes Endocrinol. 2019. PMID: 31447410 Free PMC article. No abstract available.
References
-
- Black DM, Cummings SR, Karpf DB, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 1996; 348: 1535–41. - PubMed
-
- Harris ST, Watts NB, Genant HK, et al. Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA 1999; 282: 134–52. - PubMed
-
- Ettinger B, Black DM, Mitlak BH, et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA 1999; 282: 637–45. - PubMed
-
- Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001; 344: 1434–41. - PubMed
-
- Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med 2009; 361: 756–65. - PubMed
