

Syncope and Twitching at the Emergency Department
- PMID: 31447480
- PMCID: PMC6730258
- DOI: 10.12659/AJCR.916945
Syncope and Twitching at the Emergency Department
Abstract
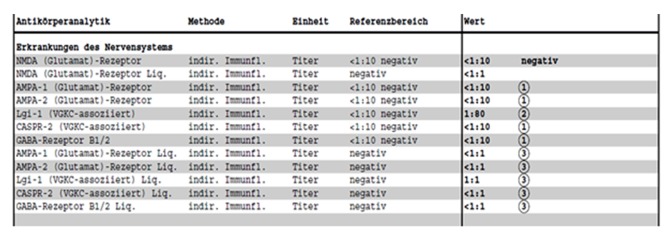
BACKGROUND Anti-LGI1 encephalitis is a type of autoimmune limbic encephalitis. This case report elucidates features of anti-LGI1 limbic encephalitis, focusing on clinical findings and outcome as well as on rarely reported sinus arrest and its pathophysiology. CASE REPORT A 49-year-old female patient presented at the Emergency Department (ED) because of twitching and an acute confusional state. Initial neurological examination revealed cognitive disturbance with disorientation, inattention, and amnestic deficits. While in the ED, twitching of the right arm was observed and shortly thereafter she experienced a sinus arrest. A temporary cardiac pacemaker was implanted. Laboratory investigations demonstrated mild hyponatremia and positive LGI1-IgG antibodies in serum. An initial head MRI was unremarkable and electroencephalography showed epileptic seizure activity starting focally in the left hemisphere synchronous with the intermittent twitching of the right arm. A seizure-suppressant therapy with levetiracetam, valproate, and gabapentin was initiated, as well as an immunosuppressive pulse therapy with methylprednisolone followed by a tapering oral regimen of prednisolone. Within a few days, the seizures ceased. One month later, neurocognitive test results were back to normal. At 2 years, mild depressive symptoms and anxiety disorder were the main clinical problems, as well as episodic migraine-like headaches. CONCLUSIONS Repetitive focal dystonic seizures, confusion, amnestic deficits, sinus arrest, and mild-to-moderate hyponatremia are pathognomonic features of anti-LGI1 limbic encephalitis. Sinus arrest may occur because of a direct pathophysiological dysfunction of the structures involved in autonomic cardiac rhythm control or as an ictal or postictal phenomenon. Early diagnosis and initiation of immunosuppressive therapy are both of utmost importance for favorable clinical outcome.
Conflict of interest statement
None.
Figures



References
-
- Van Sonderen A, Thijs RD, Coenders EC, et al. Anti-LGI1 encephalitis, clinical syndrome and long-term follow-up. Neurology. 2016;87:1449–56. - PubMed
-
- Navarro V, Kas A, Apartis E, et al. Motor cortex and hippocampus are the two main cortical targets in LGI1-antibody encephalitis. Brain. 2016;139:1079–93. - PubMed
-
- Irani SR, Buckley C, Vincent A, et al. Immunotherapy-responsive seizure-like episodes with potassium channel antibodies. Neurology. 2008;71:1647–48. - PubMed
