

Does Routine Anti-Osteoporosis Medication Lower the Risk of Fractures in Male Subjects? An Updated Systematic Review With Meta-Analysis of Clinical Trials
- PMID: 31447677
- PMCID: PMC6695469
- DOI: 10.3389/fphar.2019.00882
Does Routine Anti-Osteoporosis Medication Lower the Risk of Fractures in Male Subjects? An Updated Systematic Review With Meta-Analysis of Clinical Trials
Abstract
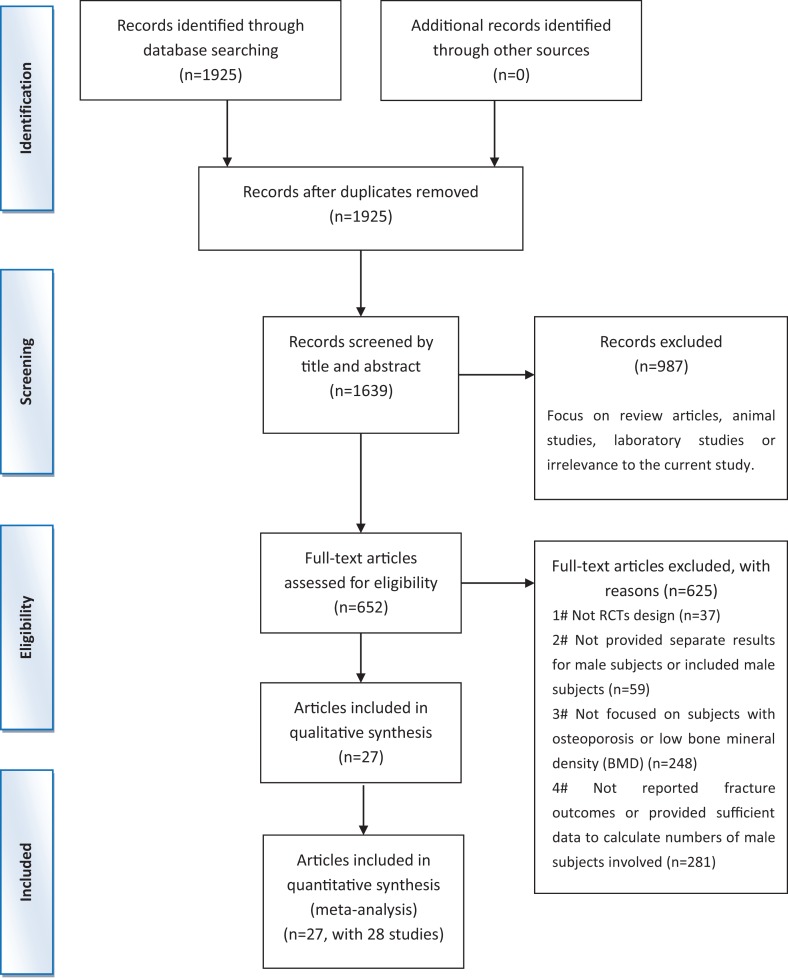
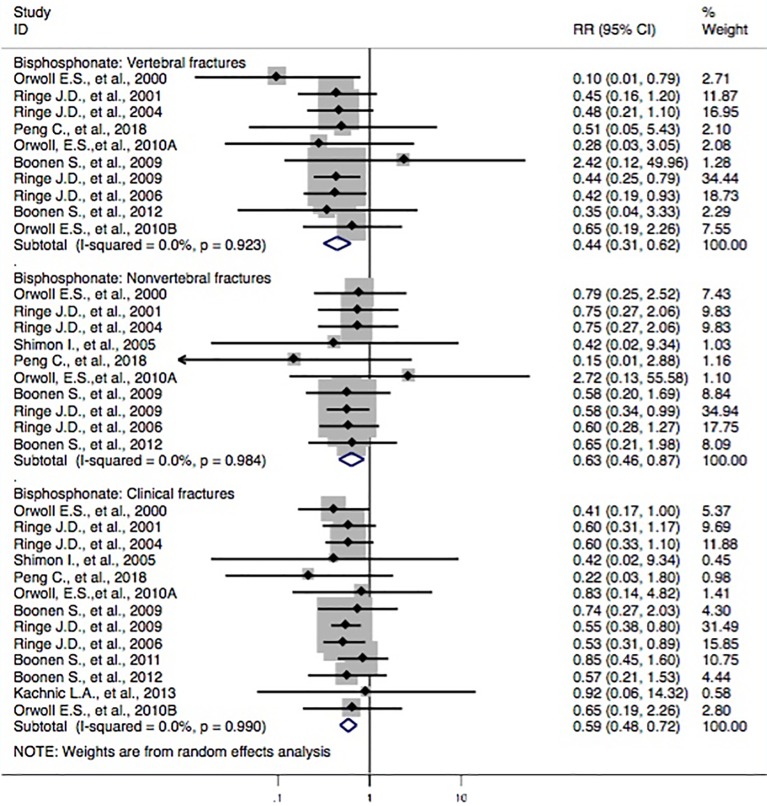
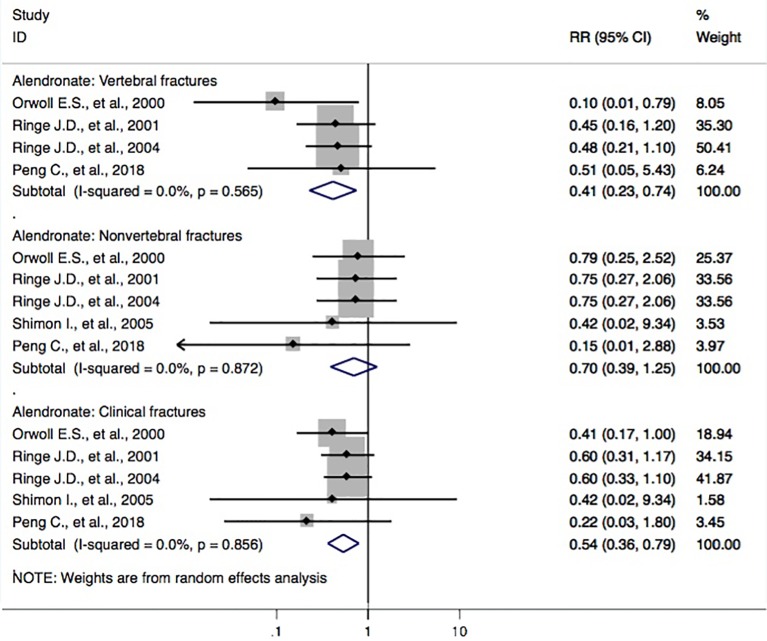
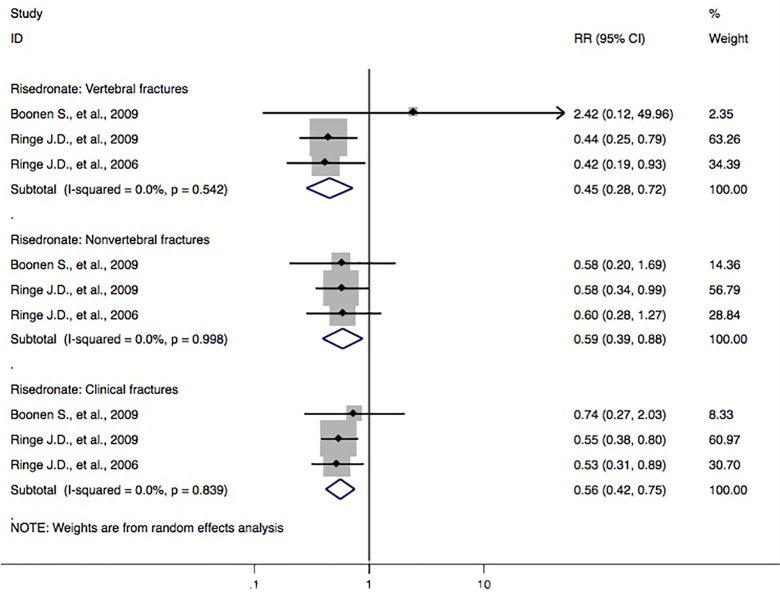
Background: Several epidemiological articles have reported the correlations between anti-osteoporosis medication and the risks of fractures in male and female subjects, but the specific efficacy of anti-osteoporosis medication for male subjects remains largely unexplored. Objective: The aim of this study was to evaluate the correlation between anti-osteoporosis medication and the risk of fracture in relation to low bone mass [including outcomes of osteoporosis, fracture, and bone mineral density (BMD) loss] in male subjects analyzed in studies within the updated literature. Methods: Randomized controlled trials (RCTs) that analyzed the effectiveness of a treating prescription for male subjects with osteoporosis (or low BMD) and that focused on the outcomes of fracture were included. Relevant studies from Embase, Web of Science, PubMed, and Chinese database of CNKI were retrieved from inception to January 30th, 2019. Two staff members carried out the eligibility assessment and data extraction. The discrepancies were settled by consultation with another researcher. We calculated the pooled relative risks (RRs) based on 95% confidence intervals (CIs). Results: Twenty-seven documents (28 studies) with 5,678 subjects were identified. For the category of bisphosphonates, significant results were observed in pooled analyses for decreased risk of the vertebral fracture domain (RR, 0.44 [95% CI, 0.31-0.62]), nonvertebral fracture domain (RR, 0.63 [95% CI, 0.46-0.87]), and clinical fracture domain (RR, 0.59 [95% CI, 0.48-0.72]) compared with those of controls. Participants with bisphosphonates had a 56% (95% CI = 38-69%) lower risk of vertebral fractures, 37% (95% CI = 13-54%) lower risk of nonvertebral fractures, and 41% (95% CI = 28-52%) lower risk of clinical fractures. Furthermore, meta-analyses also demonstrated a decreased risk of the vertebral fracture domain via treatment with risedronate (RR, 0.45 [95% CI, 0.28-0.72]) and alendronate (RR, 0.41 [95% CI, 0.23-0.74]), but not with calcitriol, calcitonin, denosumab, ibandronate, monofluorophosphate, strontium ranelate, teriparatide, or zoledronic acid, compared with that of controls. Conclusions: This systematic review confirms that bisphosphonates were connected with a decreased risk of vertebral fractures, nonvertebral fractures, and clinical fractures for male subjects with osteoporosis. Future research is needed to further elucidate the role of nonbisphosphonates in treating fractures of osteoporosis subjects.
Keywords: anti-osteoporosis medication; clinical trials; literature review; osteoporotic fracture; risk reduction; routine therapy.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources