

The Utility of Near-Infrared Fluorescence and Indocyanine Green During Robotic Pulmonary Resection
- PMID: 31448283
- PMCID: PMC6696346
- DOI: 10.3389/fsurg.2019.00047
The Utility of Near-Infrared Fluorescence and Indocyanine Green During Robotic Pulmonary Resection
Abstract
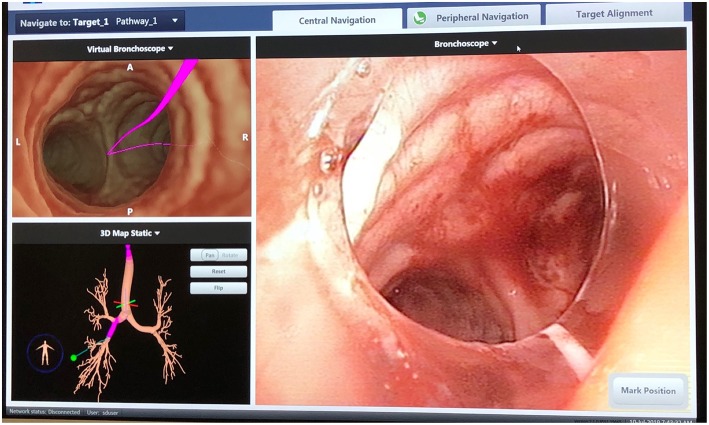
During minimally invasive pulmonary resection, it is often difficult to localize pulmonary nodules that are small (<2 cm), low-density/subsolid on imaging, or deep to the visceral pleura. The use of near-infrared fluorescence (NIF) imaging for localizing pulmonary nodules using indocyanine green (ICG) contrast is an emerging technology that is increasingly utilized during pulmonary resection. When administered via electromagnetic navigational bronchoscopy (ENB), ICG can accurately localize pulmonary nodules. When injected intravenously (IV), ICG can also help delineate the intersegmental plane. Research is ongoing regarding the utility of ICG for identification of the sentinel lymph node in lung cancer.
Keywords: electromagnetic; fluorescence; localization; lung cancer; navigational bronchoscopy; pulmonary resection; robotic.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources