

Quantifiable Bleeding in Children Supported by Extracorporeal Membrane Oxygenation and Outcome
- PMID: 31449061
- PMCID: PMC8608374
- DOI: 10.1097/CCM.0000000000003968
Quantifiable Bleeding in Children Supported by Extracorporeal Membrane Oxygenation and Outcome
Abstract
Objectives: To evaluate the association between bleeding from chest tubes and clinical outcomes in children supported by extracorporeal membrane oxygenation.
Design: Secondary analysis of a large observational cohort study.
Setting: Eight pediatric institutions within the Eunice Kennedy Shriver National Institute of Child Health and Human Development's Collaborative Pediatric Critical Care Research Network.
Patients: Critically ill children supported by extracorporeal membrane oxygenation.
Interventions: None.
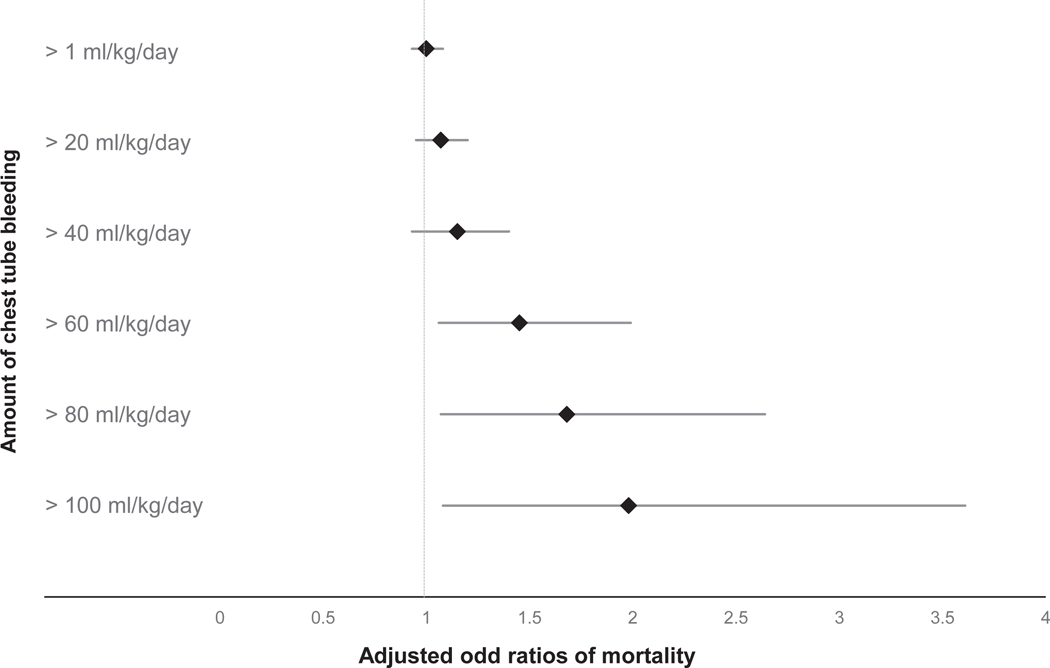
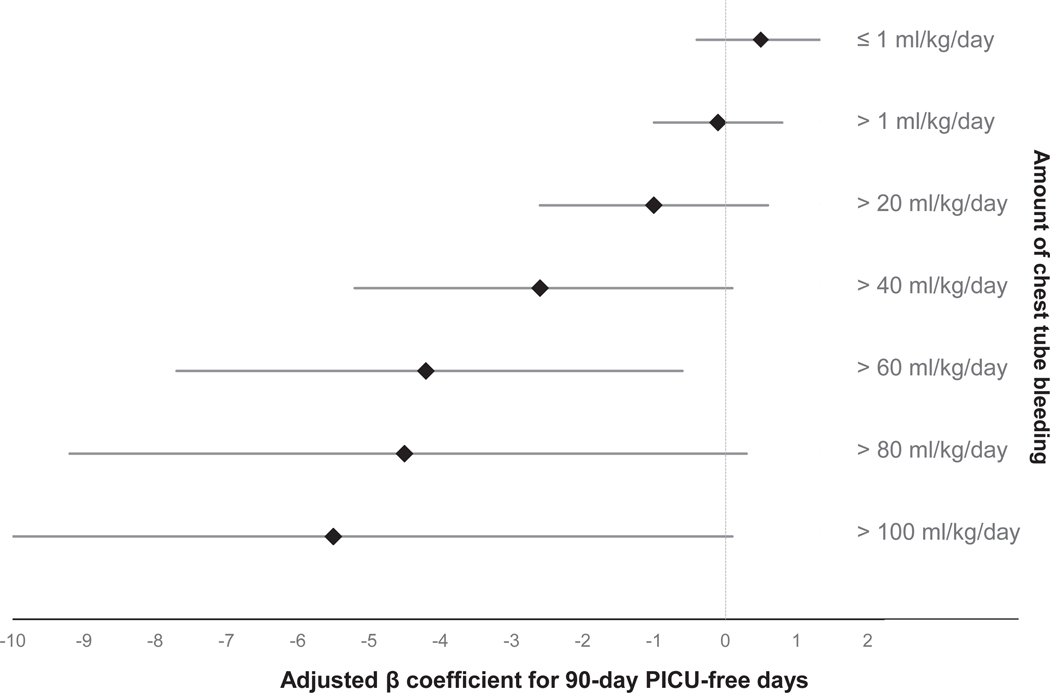
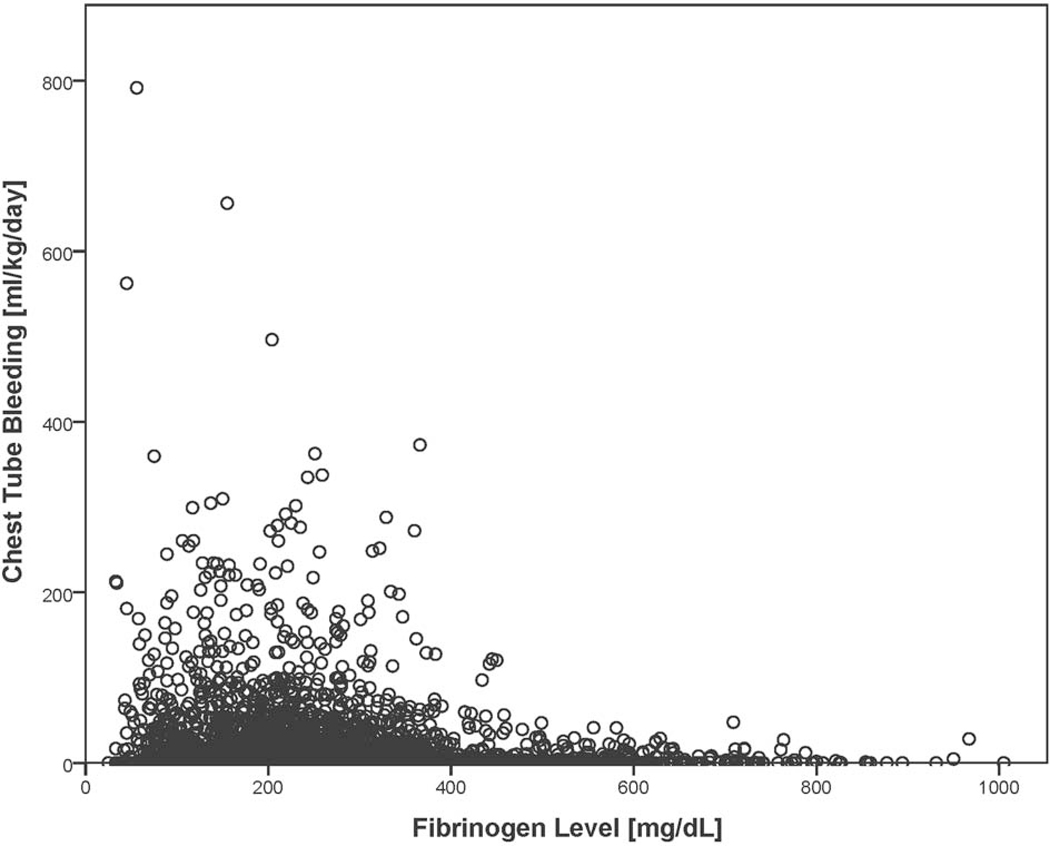
Measurements and main results: Daily chest tube bleeding, results from hemostatic assays, transfusion volumes, 90-day PICU-free days, and mortality were collected prospectively by trained bedside extracorporeal membrane oxygenation specialists and research coordinators. Extracorporeal membrane oxygenation was employed in the care of 514 consecutive patients. Sixty percent of patients had at least one episode of chest tube bleeding (median chest tube blood volume over the entire extracorporeal membrane oxygenation course was 123 mL/kg [interquartile range, 47-319 mL/kg]). Twenty-six percent had at least 1 day of bleeding from the chest tube greater than 100 mL/kg/d. The number of days with chest tube bleeding greater than 60 mL/kg/d was independently associated with increased in-hospital mortality (adjusted odds ratio, 1.43; 95% CI, 1.05-1.97; p = 0.02) and decreased PICU-free days (beta coefficient, -4.2; 95% CI, -7.7 to -0.6; p = 0.02). The total amount of bleeding from chest tube were independently associated with increased mortality (per mL/kg/extracorporeal membrane oxygenation run; adjusted odds ratio, 1.002; 95% CI, 1.000-1.003; p = 0.04). Fibrinogen, weight, indication for extracorporeal membrane oxygenation, and need for hemodialysis were independently associated with chest tube bleeding, whereas platelet count, coagulation tests, heparin dose, and thrombotic events were not.
Conclusions: In children supported by extracorporeal membrane oxygenation, chest tube bleeding above 60 mL/kg/d was independently associated with worse clinical outcome. Low fibrinogen was independently associated with chest tube bleeding, whereas platelet count and hemostatic tests were not. Further research is needed to evaluate if interventions to prevent or stop chest tube bleeding influence the clinical outcome.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Nevo S, Swan V, Enger C, et al.: Acute bleeding after bone marrow transplantation (BMT)- incidence and effect on survival. A quantitative analysis in 1,402 patients. Blood 1998, 91(4):1469–1477. - PubMed
-
- Eikelboom JW, Mehta SR, Anand SS, et al.: Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation 2006, 114(8):774–782. - PubMed
-
- Arnold DM, Donahoe L, Clarke FJ, et al.: Bleeding during critical illness: a prospective cohort study using a new measurement tool. Clinical and investigative medicine Medecine clinique et experimentale 2007, 30(2):E93–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
