

Risk Factors and Outcomes Associated With Treatment of Asymptomatic Bacteriuria in Hospitalized Patients
- PMID: 31449295
- PMCID: PMC6714039
- DOI: 10.1001/jamainternmed.2019.2871
Risk Factors and Outcomes Associated With Treatment of Asymptomatic Bacteriuria in Hospitalized Patients
Abstract
Importance: Treatment of asymptomatic bacteriuria (ASB) with antibiotics is a common factor in inappropriate antibiotic use, but risk factors and outcomes associated with treatment of ASB in hospitalized patients are not well defined.
Objective: To evaluate factors associated with treatment of ASB among hospitalized patients and the possible association between treatment and clinical outcomes.
Design, setting, and participants: A retrospective cohort study was conducted from January 1, 2016, through February 1, 2018, at 46 hospitals participating in the Michigan Hospital Medicine Safety Consortium. A total of 2733 hospitalized medical patients with ASB, defined as a positive urine culture without any documented signs or symptoms attributable to urinary tract infection, were included in the analysis.
Exposures: One or more antibiotic dose for treatment of ASB.
Main outcomes and measures: Estimators of antibiotic treatment of ASB. Secondary outcomes included 30-day mortality, 30-day hospital readmission, 30-day emergency department visit, discharge to post-acute care settings, Clostridioides difficile infection (formerly known as Clostridium difficile) at 30 days, and duration of hospitalization after urine testing.
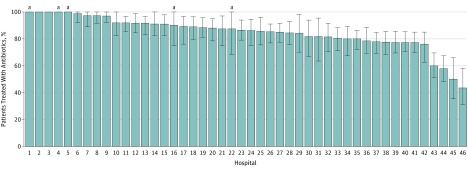
Results: Of 2733 patients with ASB, 2138 were women (78.2%); median age was 77 years (interquartile range [IQR], 66-86 years). A total of 2259 patients (82.7%) were treated with antibiotics for a median of 7 days (IQR, 4-9 days). Factors associated with ASB treatment included older age (odds ratio [OR], 1.10 per 10-year increase; 95% CI, 1.02-1.18), dementia (OR, 1.57; 95% CI, 1.15-2.13), acutely altered mental status (OR, 1.93; 95% CI, 1.23-3.04), urinary incontinence (OR, 1.81; 95% CI, 1.36-2.41), leukocytosis (white blood cell count >10 000/μL) (OR, 1.55; 95% CI, 1.21-2.00), positive urinalysis (presence of leukocyte esterase or nitrite, or >5 white blood cells per high-power field) (OR, 2.83; 95% CI, 2.05-3.93), and urine culture with a bacterial colony count greater than 100 000 colony-forming units per high-power field (OR, 2.30; 95% CI, 1.83-2.91). Treatment of ASB was associated with longer duration of hospitalization after urine testing (4 vs 3 days; relative risk, 1.37; 95% CI, 1.28-1.47). No other differences in secondary outcomes were identified after propensity weighting.
Conclusions and relevance: Hospitalized patients with ASB commonly receive inappropriate antibiotic therapy. Antibiotic treatment did not appear to be associated with improved outcomes; rather, treatment may be associated with longer duration of hospitalization after urine testing. To possibly reduce inappropriate antibiotic use, stewardship efforts should focus on improving urine testing practices and management strategies for elderly patients with altered mental status.
Conflict of interest statement
Figures
References
-
- Magill SS, Edwards JR, Beldavs ZG, et al. ; Emerging Infections Program Healthcare-Associated Infections and Antimicrobial Use Prevalence Survey Team . Prevalence of antimicrobial use in US acute care hospitals, May-September 2011. JAMA. 2014;312(14):1438-1446. doi:10.1001/jama.2014.12923 - DOI - PMC - PubMed
-
- Nicolle LE, Bradley S, Colgan R, Rice JC, Schaeffer A, Hooton TM; Infectious Diseases Society of America; American Society of Nephrology; American Geriatric Society . Infectious Diseases Society of America guidelines for the diagnosis and treatment of asymptomatic bacteriuria in adults. Clin Infect Dis. 2005;40(5):643-654. doi:10.1086/427507 - DOI - PubMed
