

Paradoxical reactions in Buruli ulcer after initiation of antibiotic therapy: Relationship to bacterial load
- PMID: 31449522
- PMCID: PMC6709892
- DOI: 10.1371/journal.pntd.0007689
Paradoxical reactions in Buruli ulcer after initiation of antibiotic therapy: Relationship to bacterial load
Abstract
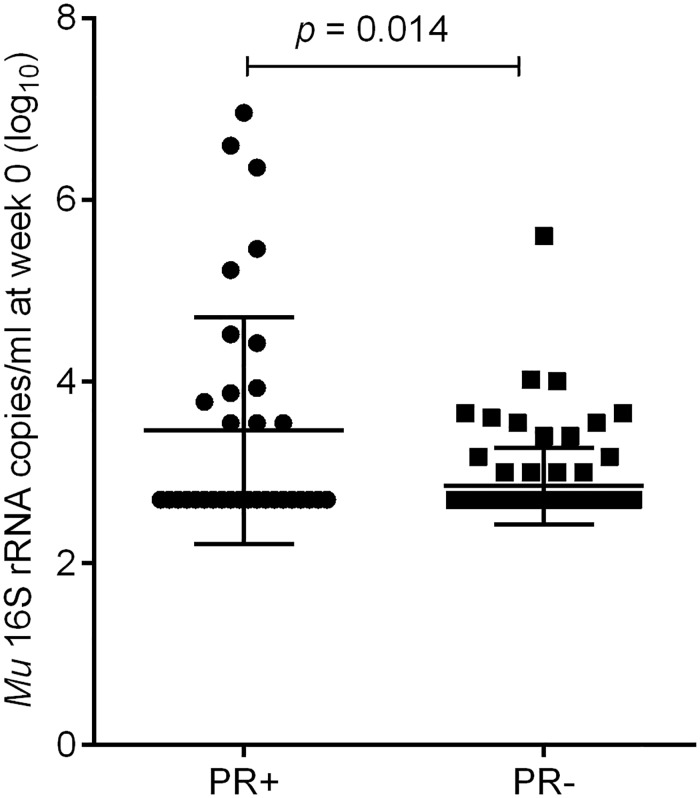
Background: We investigated the relationship between bacterial load in Buruli ulcer (BU) lesions and the development of paradoxical reaction following initiation of antibiotic treatment.
Methods: This was a longitudinal study involving BU patients from June 2013 to June 2017. Fine needle aspirates (FNA) and swab samples were obtained to establish the diagnosis of BU by PCR. Additional samples were obtained at baseline, during and after treatment (if the lesion had not healed) for microscopy, culture and combined 16S rRNA reverse transcriptase/ IS2404 qPCR assay. Patients were followed up at regular intervals until complete healing.
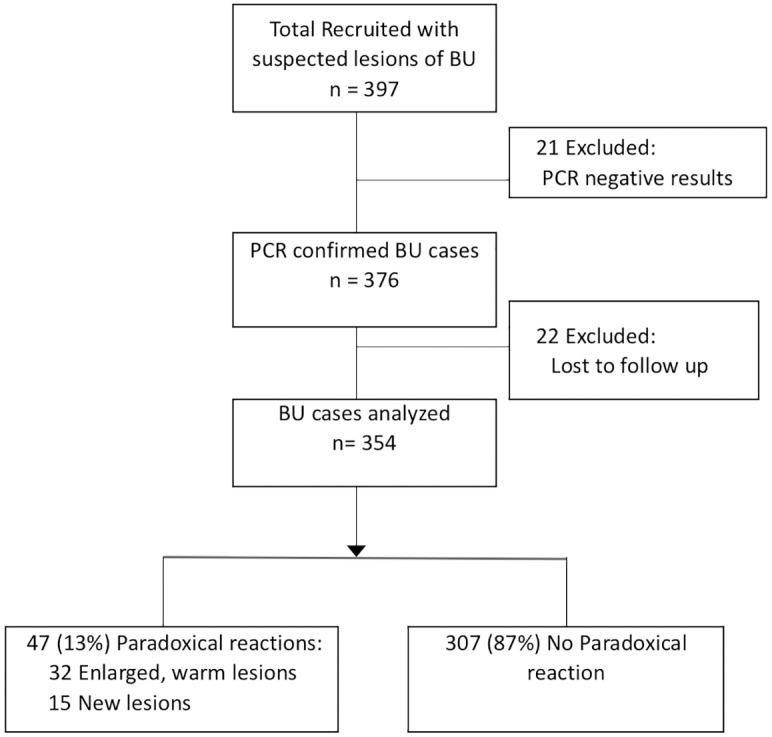
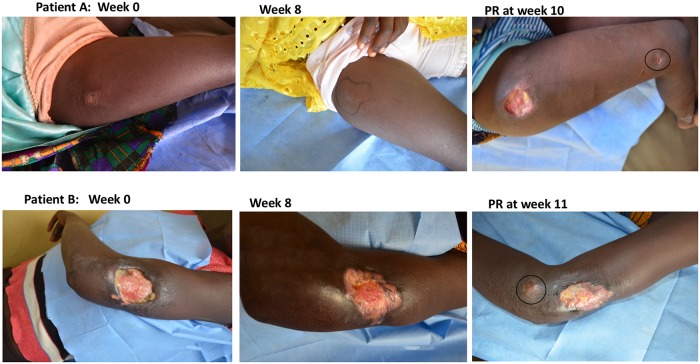
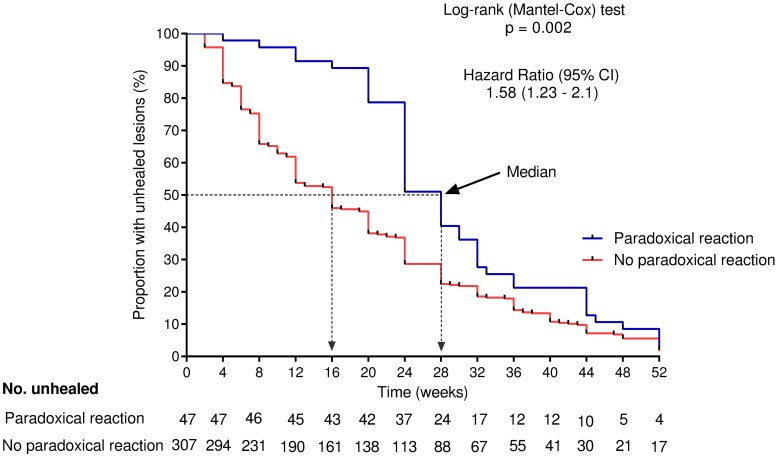
Results: Forty-seven of 354 patients (13%) with PCR confirmed BU had a PR, occurring between 2 and 42 (median 6) weeks after treatment initiation. The bacterial load, the proportion of patients with positive M. ulcerans culture (15/34 (44%) vs 29/119 (24%), p = 0.025) and the proportion with positive microscopy results (19/31 (61%) vs 28/90 (31%), p = 0.003) before initiation of treatment were significantly higher in the PR compared to the no PR group. Plaques (OR 5.12; 95% CI 2.26-11.61; p<0.001), oedematous (OR 4.23; 95% CI 1.43-12.5; p = 0.009) and category II lesions (OR 2.26; 95% CI 1.14-4.48; p = 0.02) were strongly associated with the occurrence of PR. The median time to complete healing (28 vs 13 weeks, p <0.001) was significantly longer in the PR group.
Conclusions: Buruli ulcer patients who develop PR are characterized by high bacterial load in lesion samples taken at baseline and a higher rate of positive M. ulcerans culture. Occurrence of a PR was associated with delayed healing.
Trial registration: ClinicalTrials.gov NCT02153034.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. WHO Buruli ulcer (Mycobacterium ulcerans infection). Fact sheet N° 199. Geneva, Switzerland: WHO Health Organisation; updated 2017. Geneva, Switzerland2018 [updated 16 April 2018; cited 2018 23/11/2018]. http://www.whoint/mediacentre/factsheets/fs199/en.
-
- Abass KM, Van Der Werf TS, Phillips RO, Sarfo FS, Abotsi J, Mireku SO, et al. Buruli ulcer control in a highly endemic district in Ghana: role of community-based surveillance volunteers. The American journal of tropical medicine and hygiene. 2015;92(1):115–7. 10.4269/ajtmh.14-0405 - DOI - PMC - PubMed
-
- Wansbrough-Jones M, Phillips R. Buruli ulcer: emerging from obscurity. The Lancet. 2006;367(9525):1849–58. - PubMed
-
- Ruf M-T, Chauty A, Adeye A, Ardant M-F, Koussemou H, Johnson RC, et al. Secondary Buruli Ulcer Skin Lesions Emerging Several Months after Completion of Chemotherapy: Paradoxical Reaction or Evidence for Immune Protection? PLOS Neglected Tropical Diseases. 2011;5(8):e1252 10.1371/journal.pntd.0001252 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
