

Age and Sex Estimation Using Artificial Intelligence From Standard 12-Lead ECGs
- PMID: 31450977
- PMCID: PMC7661045
- DOI: 10.1161/CIRCEP.119.007284
Age and Sex Estimation Using Artificial Intelligence From Standard 12-Lead ECGs
Abstract
Background: Sex and age have long been known to affect the ECG. Several biologic variables and anatomic factors may contribute to sex and age-related differences on the ECG. We hypothesized that a convolutional neural network (CNN) could be trained through a process called deep learning to predict a person's age and self-reported sex using only 12-lead ECG signals. We further hypothesized that discrepancies between CNN-predicted age and chronological age may serve as a physiological measure of health.
Methods: We trained CNNs using 10-second samples of 12-lead ECG signals from 499 727 patients to predict sex and age. The networks were tested on a separate cohort of 275 056 patients. Subsequently, 100 randomly selected patients with multiple ECGs over the course of decades were identified to assess within-individual accuracy of CNN age estimation.
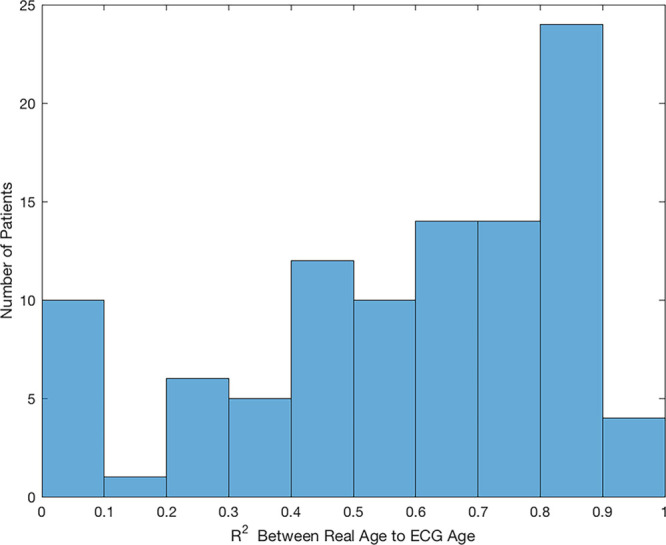
Results: Of 275 056 patients tested, 52% were males and mean age was 58.6±16.2 years. For sex classification, the model obtained 90.4% classification accuracy with an area under the curve of 0.97 in the independent test data. Age was estimated as a continuous variable with an average error of 6.9±5.6 years (R-squared =0.7). Among 100 patients with multiple ECGs over the course of at least 2 decades of life, most patients (51%) had an average error between real age and CNN-predicted age of <7 years. Major factors seen among patients with a CNN-predicted age that exceeded chronologic age by >7 years included: low ejection fraction, hypertension, and coronary disease (P<0.01). In the 27% of patients where correlation was >0.8 between CNN-predicted and chronologic age, no incident events occurred over follow-up (33±12 years).
Conclusions: Applying artificial intelligence to the ECG allows prediction of patient sex and estimation of age. The ability of an artificial intelligence algorithm to determine physiological age, with further validation, may serve as a measure of overall health.
Keywords: artificial intelligence; coronary disease; electrocardiography; hypertension; neural network.
Figures






References
-
- Holmvang L, Lüscher MS, Clemmensen P, Thygesen K, Grande P. Very early risk stratification using combined ECG and biochemical assessment in patients with unstable coronary artery disease (A thrombin inhibition in myocardial ischemia [TRIM] substudy). The TRIM Study Group. Circulation. 1998;98:2004–2009. doi: 10.1161/01.cir.98.19.2004. - PubMed
-
- Voss A, Dietz R, Fiehring H, Kleiner HJ, Kurths J, Saparin P, Vossing HJ, Witt A. High resolution ECG, heart rate variability and nonlinear dynamics: tools for high risk stratification.. Proceedings of Computers in Cardiology Conference; 1993. pp. 261–264.
-
- Attia ZI, DeSimone CV, Dillon JJ, Sapir Y, Somers VK, Dugan JL, Bruce CJ, Ackerman MJ, Asirvatham SJ, Striemer BL, Bukartyk J, Scott CG, Bennet KE, Ladewig DJ, Gilles EJ, Sadot D, Geva AB, Friedman PA. Novel bloodless potassium determination using a signal-processed single-lead ECG. J Am Heart Assoc. 2016;5:e002746. - PMC - PubMed
-
- Attia ZI, Kapa S, Lopez-Jimenez F, McKie PM, Ladewig DJ, Satam G, Pellikka PA, Enriquez-Sarano M, Noseworthy PA, Munger TM, Asirvatham SJ, Scott CG, Carter RE, Friedman PA. Screening for cardiac contractile dysfunction using an artificial intelligence-enabled electrocardiogram. Nat Med. 2019;25:70–74. doi: 10.1038/s41591-018-0240-2. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
