

Review
doi: 10.1161/JAHA.119.012788.
Epub 2019 Aug 27.
Artificial Intelligence: Practical Primer for Clinical Research in Cardiovascular Disease
Affiliations
- PMID: 31450991
- PMCID: PMC6755846
- DOI: 10.1161/JAHA.119.012788
Item in Clipboard
Review
Artificial Intelligence: Practical Primer for Clinical Research in Cardiovascular Disease
J Am Heart Assoc.
.
No abstract available
Keywords: artificial intelligence; deep learning; machine learning; risk model; risk prediction; statistics; telemedicine.
Figures
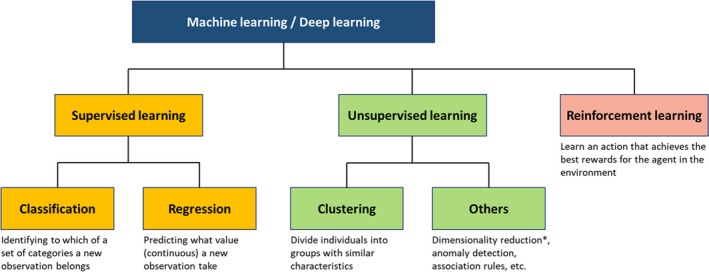
Supervised, unsupervised, and reinforcement learning. Machine learning tasks are categorized into supervised, unsupervised, or reinforcement learning. Supervised learning is used for prediction (classification or regression), whereas unsupervised learning aims to reveal hidden patterns in data. Reinforcement learning is another way of learning where an algorithm learns the best action based on its consequences, and is well suited for game theory and control theory. However, it has not had a significant role in clinical research because it requires simulating many “wrong actions” to learn. *Dimensionality reduction can also be performed in a supervised manner.
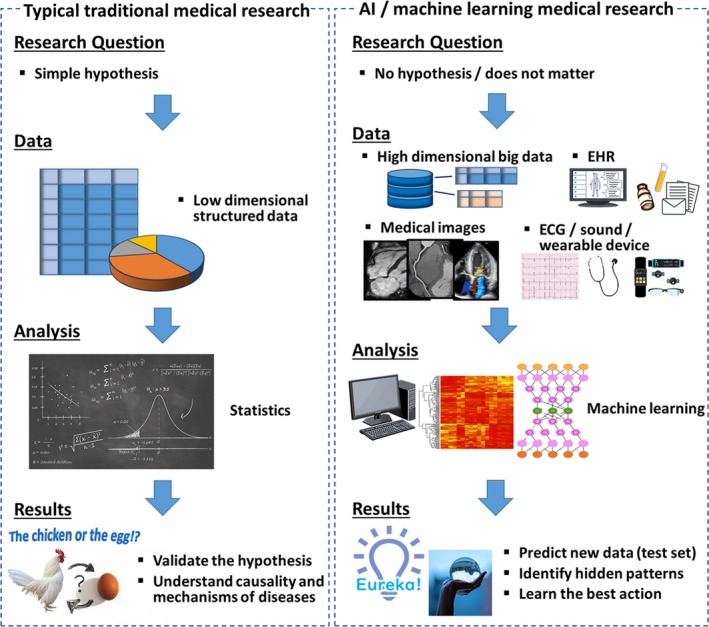
Pipelines of medical research using traditional statistics and AI . Traditional medical research formulates a hypothesis first, and tests it using statistical analysis. Medical research using AI can be hypothesis‐free and data‐driven. Compared with traditional statistics, AI can deal with various types of data, including unstructured data such as images, signals, and EHR . In contrast to traditional medical research that focuses on validation of hypotheses and understanding causality and mechanisms, the main goal of research using AI is to predict new data and identify a hidden pattern in the data. AI indicates artificial intelligence; EHR , electronic health record.
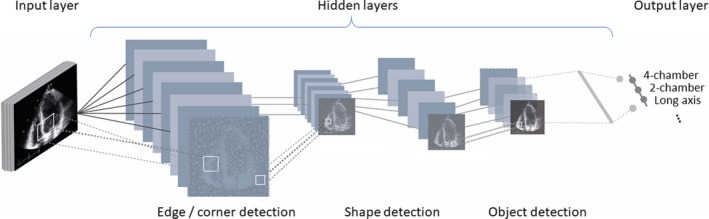
Structure of deep learning. Deep learning consists of input layers, hidden layers, and output layers. Through multiple hidden layers, raw input is gradually converted into more abstract and essential features that represent the original data. In image recognition, the input layer indicates raw pixels of the image, then first layers identify simple features of the image such as edges and lines. Succeeding layers identify somewhat more complex features such as ears, eyes, and tails. Finally, last layers recognize features of cats and dogs. As such, deep learning extracts key features from raw unstructured data and returns outputs as classification or regression.
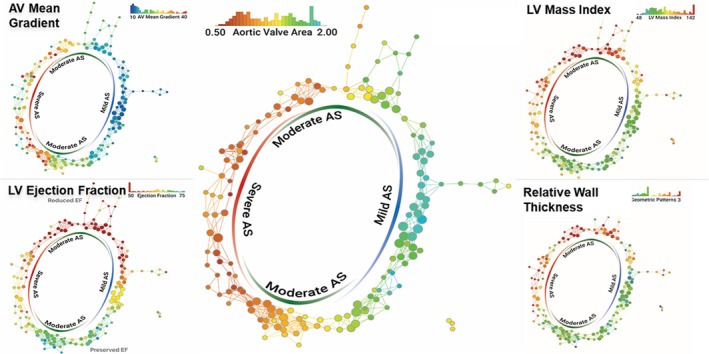
Topological data analysis in patients with AS. Topological data analysis enables integration of multidimensional complex data and visualization of hidden patterns in the data. Each node represents 1 or more patients with similar echocardiographic parameters of AS, and nodes including similar patients are connected by edges. Each panel is colored by 1 parameter written on the top right and color of the nodes represents the mean value of the parameter in the nodes. Although the network was created only from the parameters of aortic stenosis, preserved and reduced LV function (systolic and diastolic) were segregated in different regions. AS indicates aortic stenosis; AV, aortic valve; LV , left ventricle. Reprinted from Casaclang‐Verzosa et al19 with permission. Copyright ©2019, Elsevier.
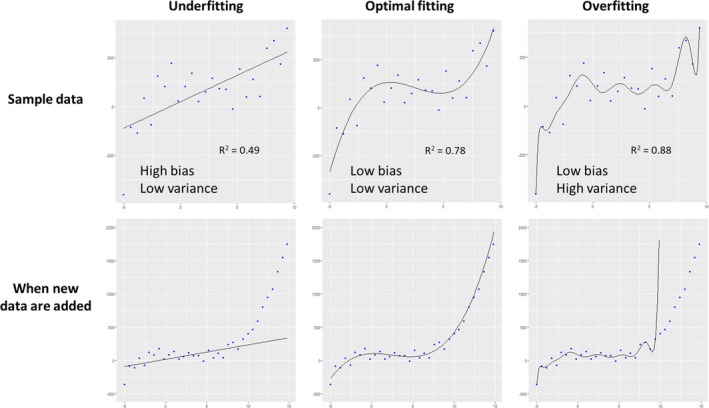
Underfitting, optimal fitting, and overfitting. The upper row shows regression models created in sample data (=training data), and new data from the same population were added in the bottom row. A simple linear model on the left panel was underfitted to the data, with low variance (ie, fluctuations in predicted value) but high bias (ie, difference between predicted and true value). In contrast, a complex model on the right panel was overfitted with low bias but high variance, because it also modeled random noise in the sample data. As a model becomes more complex, goodness‐of‐fit increases and bias decreases. However, overfitted models do not capture real association in data and cannot work well for new data.
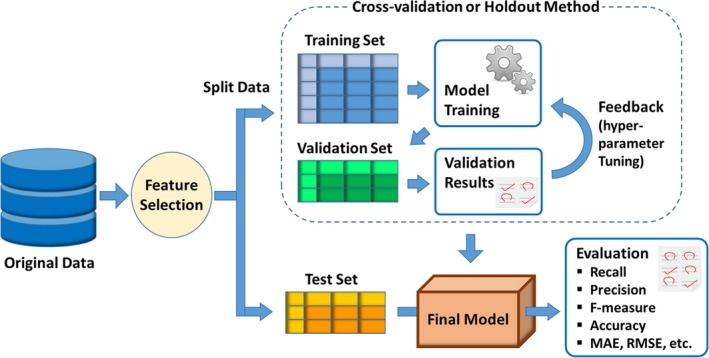
Development and evaluation of machine learning model. Since machine learning aims to predict new data in supervised learning, the test set is always preserved during when the machine learning model is built in order to guarantee generalizability. Ordinarily, the remaining data are further split into the training set, which is used to build models (calculate weights), and the validation set, which is used to validate the generated models and to tune hyperparameters. This training‐validation process is performed using a cross‐validation or holdout method. Finally, performance of the created model is evaluated using a test set that is not used in the model‐building process. MAE indicates mean absolute error; RMSE , root mean square error.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jimenez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER III, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB. Executive summary: heart disease and stroke statistics–2016 update: a report from the American Heart Association. Circulation. 2016;133:447–454. - PubMed
-
- Narula S, Shameer K, Salem Omar AM, Dudley JT, Sengupta PP. Machine‐learning algorithms to automate morphological and functional assessments in 2D echocardiography. J Am Coll Cardiol. 2016;68:2287–2295. - PubMed
-
- Mayr A, Binder H, Gefeller O, Schmid M. The evolution of boosting algorithms. From machine learning to statistical modelling. Methods Inf Med. 2014;53:419–427. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
