

Cost-utility, cost-effectiveness, and budget impact of Internet-based cognitive behavioral therapy for breast cancer survivors with treatment-induced menopausal symptoms
- PMID: 31451978
- PMCID: PMC6817759
- DOI: 10.1007/s10549-019-05410-w
Cost-utility, cost-effectiveness, and budget impact of Internet-based cognitive behavioral therapy for breast cancer survivors with treatment-induced menopausal symptoms
Abstract
Purpose: Internet-based cognitive behavioral therapy (iCBT), with and without therapist support, is effective in reducing treatment-induced menopausal symptoms and perceived impact of hot flushes and night sweats (HF/NS) in breast cancer survivors. The aim of the current study was to evaluate the cost-utility, cost-effectiveness, and budget impact of both iCBT formats compared to a waiting list control group from the Dutch healthcare perspective.
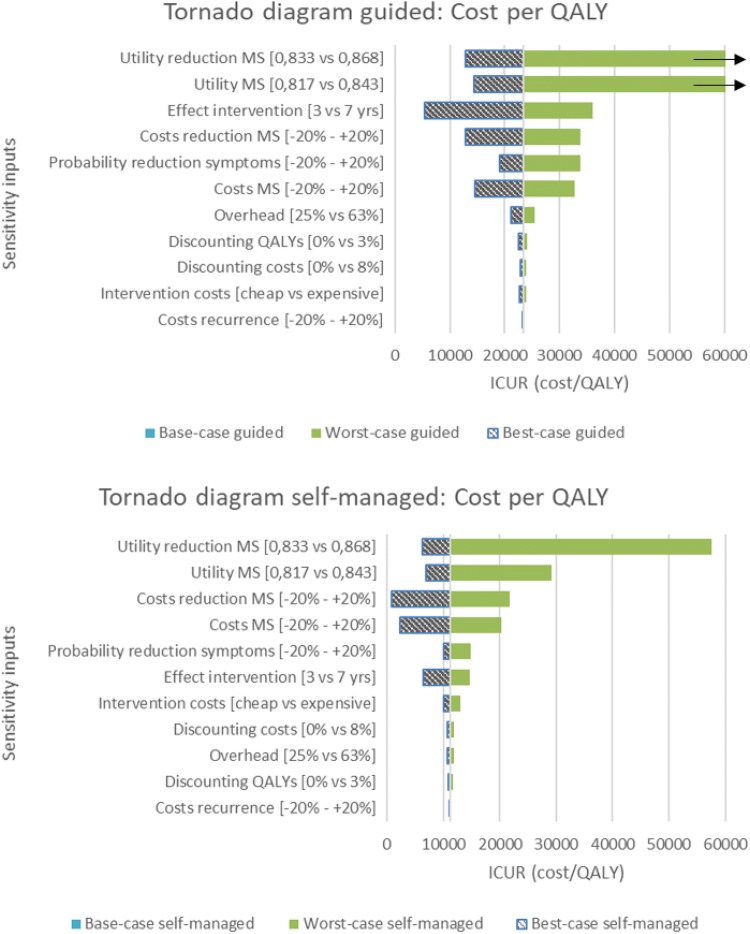
Methods: A Markov model was constructed with a 5-year time horizon. Costs and health outcomes were measured alongside a randomized controlled clinical trial and included quality-adjusted life years (QALYs), overall levels of menopausal symptoms, and perceived impact of HF/NS. Uncertainty was examined using probabilistic and deterministic sensitivity analyses, together with a scenario analysis incorporating a different perspective.
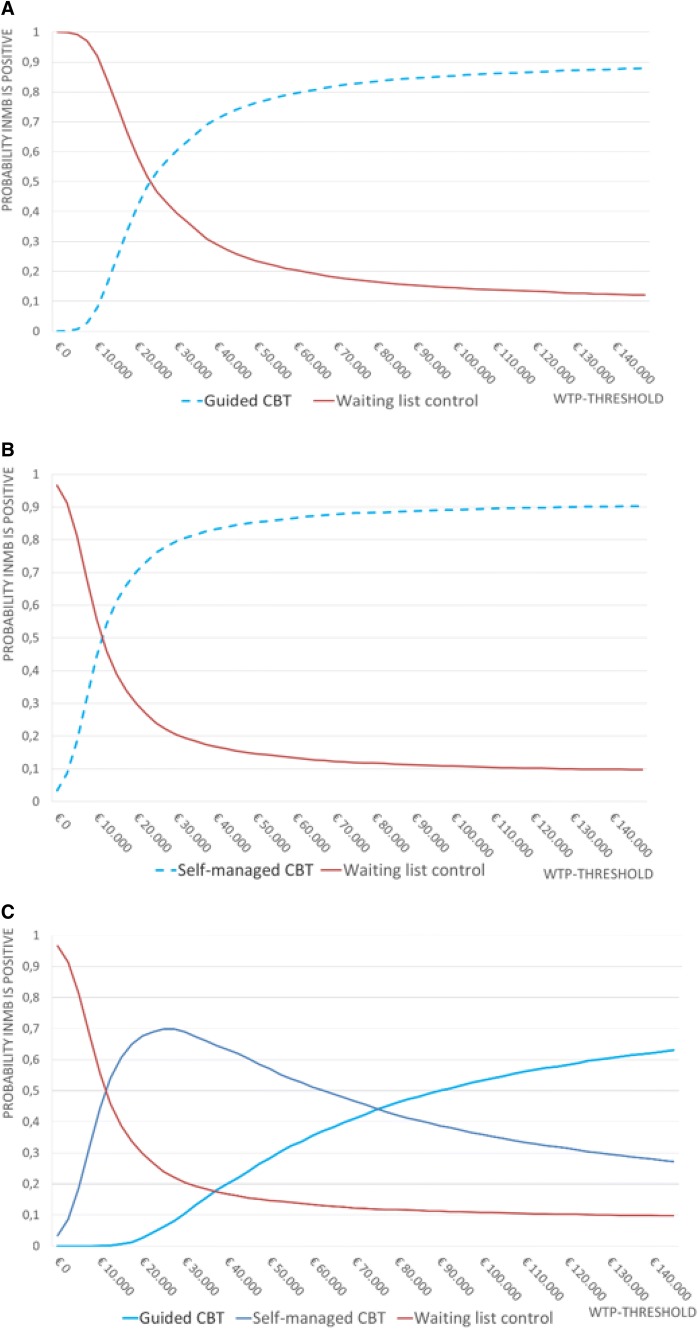
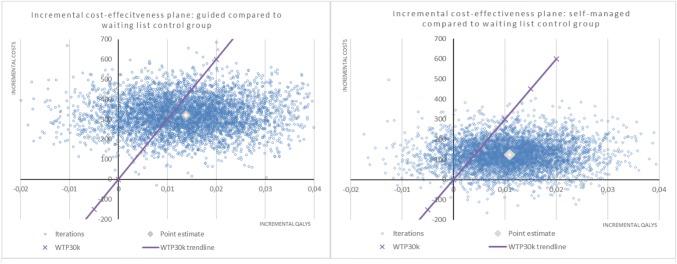
Results: iCBT was slightly more expensive than the waiting list control, but also more effective, resulting in incremental cost-utility ratios of €23,331/QALY and €11,277/QALY for the guided and self-managed formats, respectively. A significant reduction in overall levels of menopausal symptoms or perceived impact of HF/NS resulted in incremental costs between €1460 and €1525 for the guided and €500-€753 for the self-managed format. The estimated annual budget impact for the Netherlands was €192,990 for the guided and €74,592 for the self-managed format.
Conclusion: Based on the current trial data, the results indicate that both guided and self-managed iCBT are cost-effective with a willingness-to-pay threshold of well below €30,000/QALY. Additionally, self-managed iCBT is the most cost-effective strategy and has a lower impact on healthcare budgets.
Keywords: Breast cancer; Budget impact; Cognitive behavioral therapy; Cost-effectiveness; Internet-based; Menopause.
Conflict of interest statement
Myra S. Hunter declares she receives royalties from Routledge and Boom publisher. No other conflicts of interest are present and other authors declare that they have no conflict of interest.
Figures
References
-
- Bines J, Oleske DM, Cobleigh MA. Ovarian function in premenopausal women treated with adjuvant chemotherapy for breast cancer. J Clin Oncol. 1996;14(5):1718–1729. - PubMed
-
- Shapiro CL, Recht A. Side effects of adjuvant treatment of breast cancer. N Engl J Med. 2001;344(26):1997–2008. - PubMed
-
- Carpenter JS, Andrykowski MA. Menopausal symptoms in breast cancer survivors. Oncol Nurs Forum. 1999;26(8):1311–1317. - PubMed
-
- Gupta P, Sturdee DW, Palin SL, Majumder K, Fear R, Marshall T, Paterson I. Menopausal symptoms in women treated for breast cancer: the prevalence and severity of symptoms and their perceived effects on quality of life. Climacteric. 2006;9(1):49–58. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
