

The Medicare Shared Savings Program and Outcomes for Ischemic Stroke Patients: a Retrospective Cohort Study
- PMID: 31452032
- PMCID: PMC6854149
- DOI: 10.1007/s11606-019-05283-1
The Medicare Shared Savings Program and Outcomes for Ischemic Stroke Patients: a Retrospective Cohort Study
Abstract
Background: Post-stroke care delivery may be affected by provider participation in Medicare Shared Savings Program (MSSP) Accountable Care Organizations (ACOs) through systematic changes to discharge planning, care coordination, and transitional care.
Objective: To evaluate the association of MSSP with patient outcomes in the year following hospitalization for ischemic stroke.
Design: Retrospective cohort SETTING: Get With The Guidelines (GWTG)-Stroke (2010-2014) PARTICIPANTS: Hospitalizations for mild to moderate incident ischemic stroke were linked with Medicare claims for fee-for-service beneficiaries ≥ 65 years (N = 251,605).
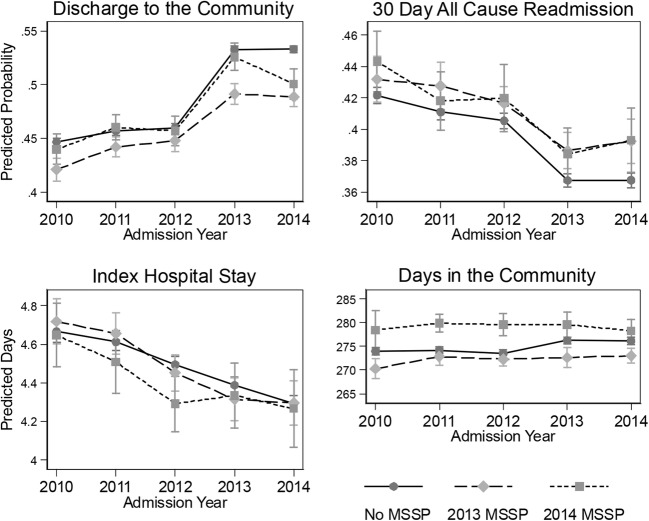
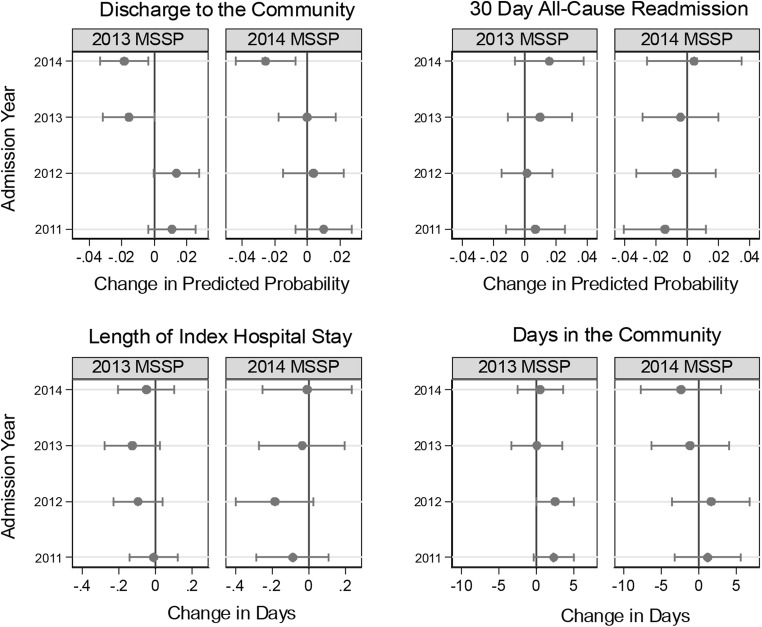
Main measures: Outcomes included discharge to home, 30-day all-cause readmission, length of index hospital stay, days in the community (home-time) at 1 year, and 1-year recurrent stroke and mortality. A difference-in-differences design was used to compare outcomes before and after hospital MSSP implementation for patients (1) discharged from hospitals that chose to participate versus not participate in MSSP or (2) assigned to an MSSP ACO versus not or both. Unique estimates for 2013 and 2014 ACOs were generated.
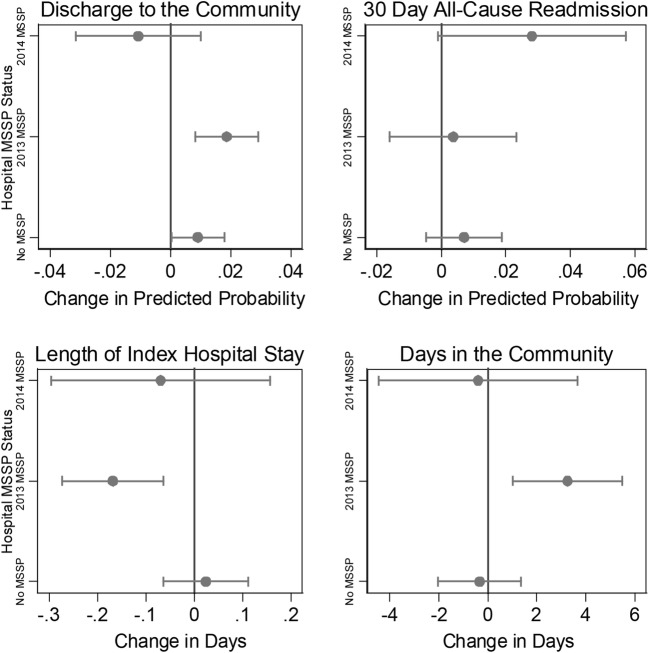
Key results: For hospitals joining MSSP in 2013 or 2014, the probability of discharge to home decreased by 2.57 (95% confidence intervals (CI) = - 4.43, - 0.71) percentage points (pp) and 1.84 pp (CI = - 3.31, - 0.37), respectively, among beneficiaries not assigned to an MSSP ACO. Among discharges from hospitals joining MSSP in 2013, beneficiary ACO alignment versus not was associated with increased home discharge, reduced length of stay, and increased home-time. For patients discharged from hospitals joining MSSP in 2014, ACO alignment was not associated with changes in utilization. No association between MSSP and recurrent stroke or mortality was observed.
Conclusions: Among patients with mild to moderate ischemic stroke, meaningful reductions in acute care utilization were observed only for ACO-aligned beneficiaries who were also discharged from a hospital initiating MSSP in 2013. Only 1 year of data was available for the 2014 MSSP cohort, and these early results suggest further study is warranted.
Registration: None.
Keywords: Medicare; health policy; health services research; outcomes; stroke; utilization.
Conflict of interest statement
ECO: Research grants from BMS, Novartis, Janssen, and GSK
GCF: Research Patient Centered Outcomes Research Institute, Consultant to Janssen
YX: Research funding from the American Heart Association, Daiichi Sankyo, Janssen Pharmaceuticals, and Genentech. Honorarium from Brain Canada
All remaining authors declare that they do not have a conflict of interest.
Figures
References
-
- McClellan M, Saunders R. Growth Of ACOs And Alternative Payment Models In 2017. Health Affairs Blog. http://www.healthaffairs.org/do/10.1377/hblog20170628.060719/full/. Published 2017. Accessed July 1, 2019. - DOI
-
- Muhlestein D, McClellan M. Accountable Care Organizations In 2016: Private And Public-Sector Growth And Dispersion. http://healthaffairs.org/blog/2016/04/21/accountable-care-organizations-.... Published 2016. July 1, 2019.
-
- Muhlestein D, Gardner P, William C, de Lisle K. Projected Growth of Accountable Care Organizations.https://leavittpartners.com/whitepaper/projected-growth-of-accountable-c... Leavitt Partners 2015. Accessed July 1, 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
