

Regenerative Therapies for Spinal Cord Injury
- PMID: 31452463
- PMCID: PMC6919264
- DOI: 10.1089/ten.TEB.2019.0182
Regenerative Therapies for Spinal Cord Injury
Abstract
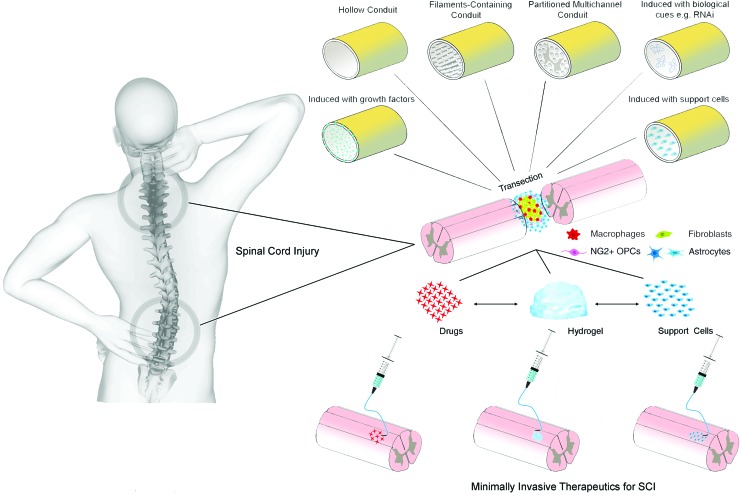
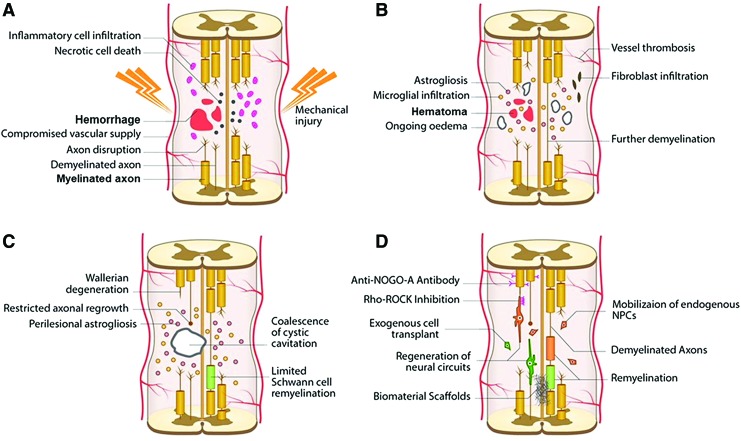
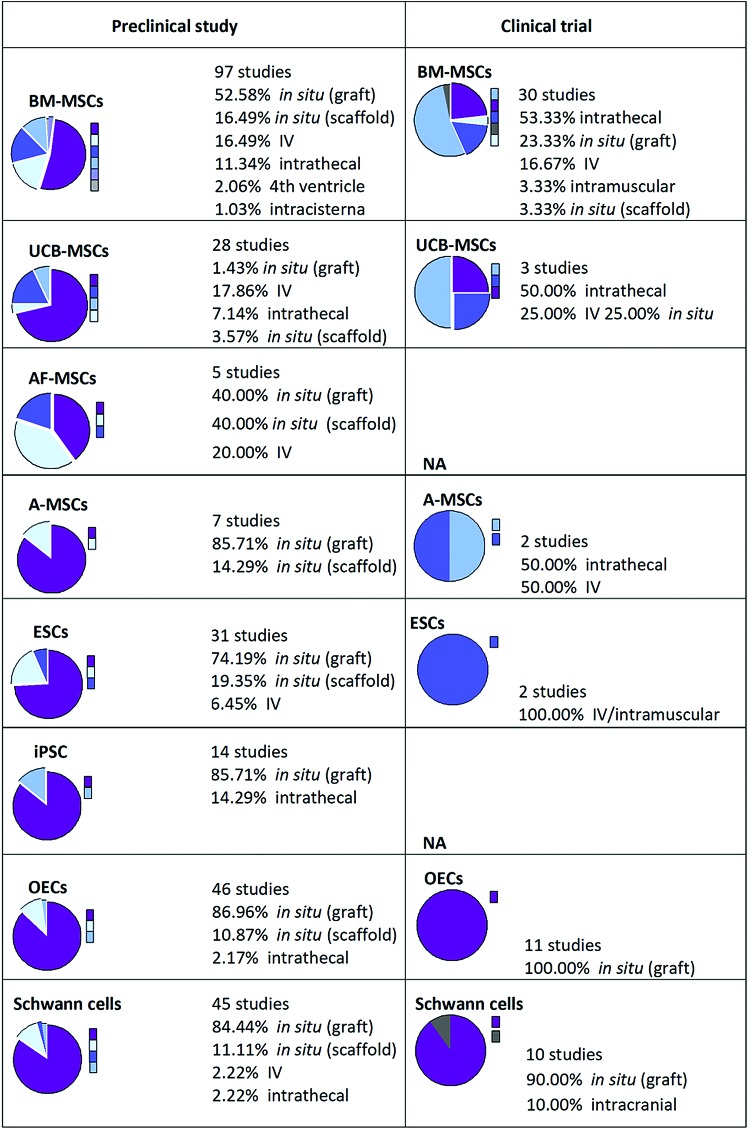
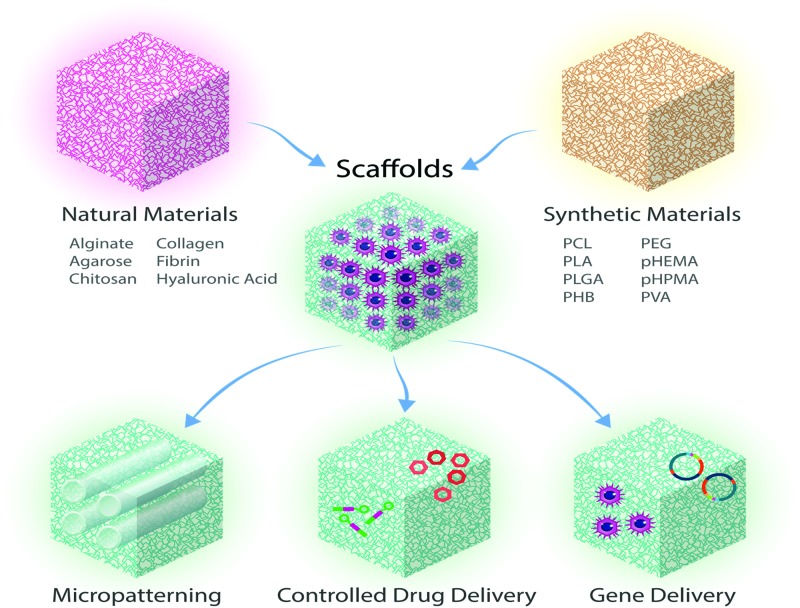
Spinal cord injury (SCI) is a serious problem that primarily affects younger and middle-aged adults at its onset. To date, no effective regenerative treatment has been developed. Over the last decade, researchers have made significant advances in stem cell technology, biomaterials, nanotechnology, and immune engineering, which may be applied as regenerative therapies for the spinal cord. Although the results of clinical trials using specific cell-based therapies have proven safe, their efficacy has not yet been demonstrated. The pathophysiology of SCI is multifaceted, complex and yet to be fully understood. Thus, combinatorial therapies that simultaneously leverage multiple approaches will likely be required to achieve satisfactory outcomes. Although combinations of biomaterials with pharmacologic agents or cells have been explored, few studies have combined these modalities in a systematic way. For most strategies, clinical translation will be facilitated by the use of minimally invasive therapies, which are the focus of this review. In addition, this review discusses previously explored therapies designed to promote neuroregeneration and neuroprotection after SCI, while highlighting present challenges and future directions. Impact Statement To date there are no effective treatments that can regenerate the spinal cord after injury. Although there have been significant preclinical advances in bioengineering and regenerative medicine over the last decade, these have not translated into effective clinical therapies for spinal cord injury. This review focuses on minimally invasive therapies, providing extensive background as well as updates on recent technological developments and current clinical trials. This review is a comprehensive resource for researchers working towards regenerative therapies for spinal cord injury that will help guide future innovation.
Keywords: biomaterials; cell therapy; minimally invasive; regeneration; spinal cord injury.
Conflict of interest statement
The authors acknowledge that they have no competing interests.
Figures
References
-
- World Health Organization; The International Spinal Cord Society. International Perspectives on Spinal Cord Injury. Geneva, Switzerland: World Health Organization, 2013
-
- Cox C.S., Jr. Cellular therapy for traumatic neurological injury. Pediatr Res 83, 325, 2018 - PubMed
-
- Jazayeri S.B., Beygi S., Shokraneh F., Hagen E.M., and Rahimi-Movaghar V.. Incidence of traumatic spinal cord injury worldwide: a systematic review. Eur Spine J 24, 905, 2015 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
