

Effectiveness of oral antibiotics for definitive therapy of non-Staphylococcal Gram-positive bacterial bloodstream infections
- PMID: 31452884
- PMCID: PMC6696838
- DOI: 10.1177/2049936119863013
Effectiveness of oral antibiotics for definitive therapy of non-Staphylococcal Gram-positive bacterial bloodstream infections
Abstract
Background: Data on the effectiveness of definitive oral (PO) antibiotics for BSIs in preparation for discharge from hospital are lacking, particularly for Gram-positive bacterial BSIs (GP-BSI). The objective of this study was to determine rates of treatment failure based on bioavailability of PO antimicrobial agents used for GP-BSI.
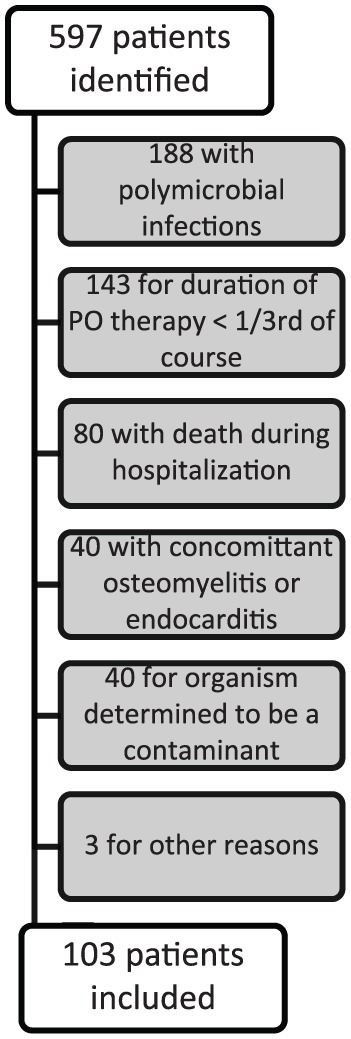
Methods: This was a single-center, retrospective cohort study of adult inpatients admitted to an academic medical center over a three-year period. Patients with a non-staphylococcal GP-BSI who received intravenous antibiotics and were then switched to PO antibiotics for at least a third of their treatment course were included. The cohort was stratified into high (⩾90%) and low (<90%) bioavailability groups. The primary endpoint was the proportion of patients experiencing clinical failure in each group. Secondary endpoints included clinical failure stratified by antibiotic group, bactericidal versus bacteriostatic PO agents, and organism.
Results: A total of 103 patients met criteria for inclusion, which failed to reach the a priori power calculation. Of the patients included, 26 received high bioavailability agents and 77 received low bioavailability agents. Infections originated largely from a pulmonary source (30%) and were caused primarily by streptococcal species (75%). Treatment failure rates were 19.2% in the high bioavailability group and 23.4% in the low bioavailability group (p = 0.66). Clinical failure stratified by subgroups also did not yield statistically significant differences.
Conclusions: Clinical failure rates were similar among patients definitively treated with high or low bioavailability agents for GP-BSI, though the study was underpowered to detect such a difference.
Keywords: Gram-positive; bacteremia; bioavailability; oral antibiotics.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
References
-
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect 2013; 19: 501–509. - PubMed
-
- Wisplinghoff H, Bischoff T, Tallent SMet al. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis 2004; 39: 309–317. - PubMed
-
- Mermel LA. Short-term peripheral venous catheter–related bloodstream infections: a systematic review. Clin Infect Dis 2017; 65: 1757–1762. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
