

Diagnosis and management of a case of retroperitoneal eosinophilic sclerosing fibroplasia in a cat
- PMID: 31452913
- PMCID: PMC6699013
- DOI: 10.1177/2055116919867178
Diagnosis and management of a case of retroperitoneal eosinophilic sclerosing fibroplasia in a cat
Abstract
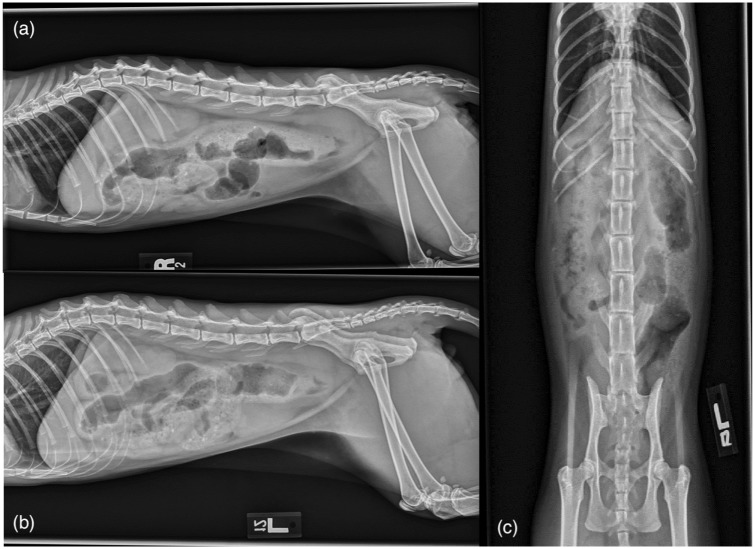
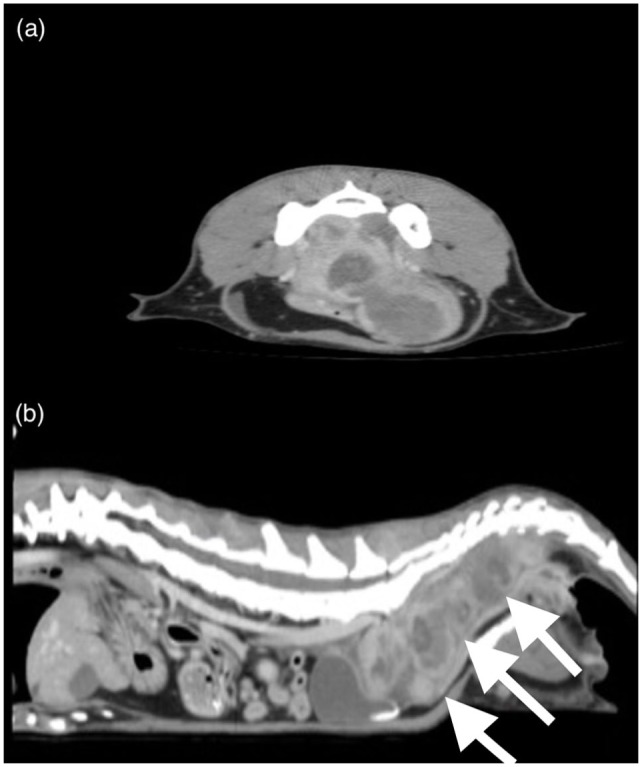
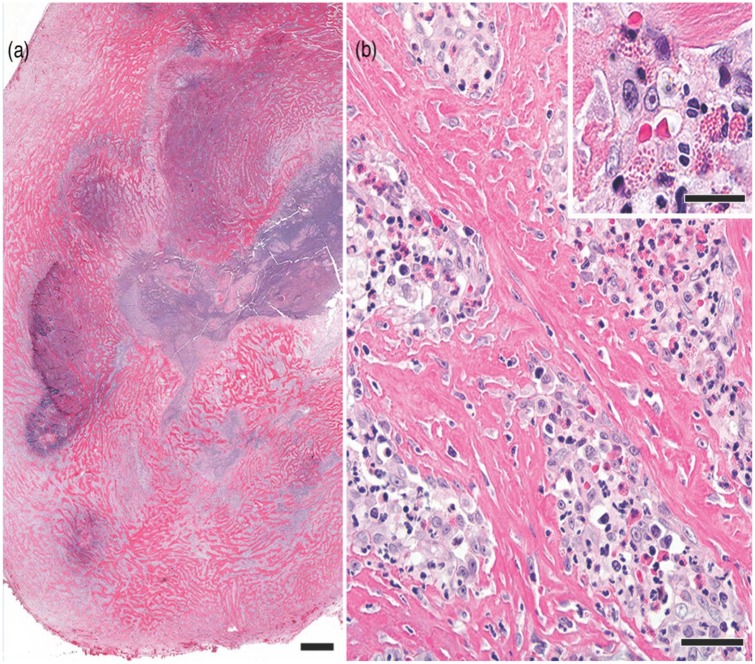
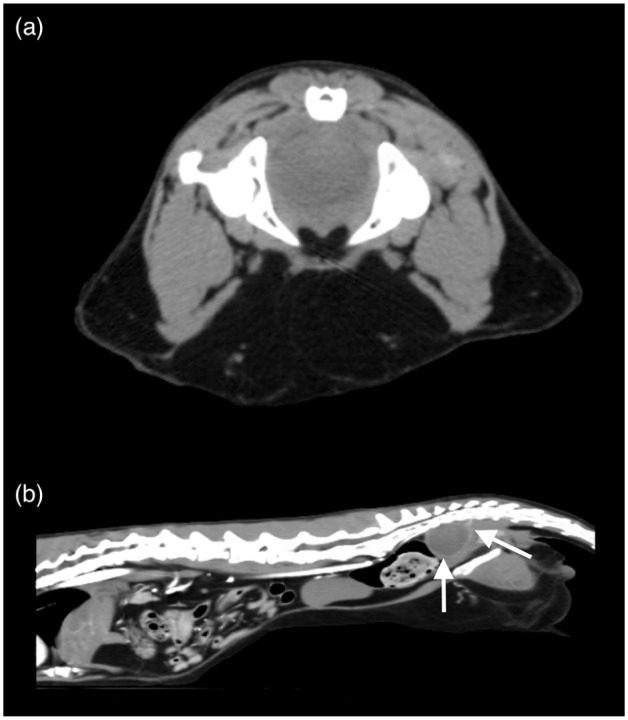
Case summary: A 4-year-old neutered male cat was presented with a 2-month history of intermittent constipation that progressed to obstipation. Primary clinical findings included a large, multi lobulated mass in the caudodorsal abdomen, peripheral eosinophilia and hyperglobulinemia. Abdominal imaging revealed a multilobulated, cavitated mass in the sublumbar region. Exploratory celiotomy revealed multiple firm masses in the sublumbar retroperitoneal space causing ventral displacement and compression of the descending colon with extension of the masses into the pelvic canal. Histopathology was consistent with feline gastrointestinal eosinophilic sclerosing fibroplasia (FGESF). Aerobic culture was positive for Staphylococcus aureus. The cat was treated with prednisolone (2 mg/kg PO q24h), lactulose (0.5 g/kg PO q8h), amoxicillin/clavulanic acid (62.5 mg/cat PO q12h for 1 month) and fenbendazole (50 mg/kg PO q24h for 5 days). Six months postoperatively, the cat had no recurrence of clinical signs. Repeat evaluation and imaging at day 732 postoperatively revealed marked improvement of the abdominal mass, resolution of peripheral eosinophilia and no clinical signs with continued prednisolone therapy (0.5 mg/kg PO q24h).
Relevance and novel information: This is a report of a primary extramural FGESF lesion, and the first description of characteristics of FGESF on CT. Previous evidence suggests that the most favorable outcomes require immunosuppressive therapy and complete surgical excision; however, this case demonstrates a favorable outcome with medical management alone.
Keywords: Gastrointestinal; eosinophilic sclerosing fibroplasia; medical; surgery.
Conflict of interest statement
Conflict of interest: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Craig LE, Hardam EE, Hertzke DMet al. Feline gastrointestinal eosinophilic sclerosing fibroplasia. Vet Pathol 2009; 46: 63–70. - PubMed
-
- Grau-Roma L, Galindo-Cardiel I, Isidoro-Ayza Met al. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia associated with phycomycetes. J Comp Pathol 2014; 151: 318–321. - PubMed
-
- Munday J, Martinez A, Soo M. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia mimicking metastatic neoplasia. N Z Vet J 2014; 62: 356–360. - PubMed
-
- Sihvo HK, Simola OT, Vainionpaa MHet al. Pathology in practice. Severe chronic multifocal intramural fibrosing and eosinophilic enteritis, with occasional intralesional bacteria, consistent with feline gastrointestinal eosinophilic sclerosing fibroplasia. J Am Vet Med Assoc 2011; 238: 585–587. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous