

Is the Width of a Surgical Margin Associated with the Outcome of Disease in Patients with Peripheral Chondrosarcoma of the Pelvis? A Multicenter Study
- PMID: 31453886
- PMCID: PMC6903848
- DOI: 10.1097/CORR.0000000000000926
Is the Width of a Surgical Margin Associated with the Outcome of Disease in Patients with Peripheral Chondrosarcoma of the Pelvis? A Multicenter Study
Abstract
Background: We attempted to resect peripheral chondrosarcoma of the pelvis with clear margins. Because of the proximity of vessels or organs, there is still concern that narrow surgical margins may have an adverse effect on disease outcomes. Although current guidelines recommend resection of histologic Grade II or Grade III chondrosarcomas with a "wide" margin, there are no specific recommendations for the adequate width of a surgical margin.
Questions/purposes: (1) What is the disease-specific and local recurrence-free survival of patients with peripheral chondrosarcoma of the pelvis treated with resection or amputation? (2) Is the width of a surgical margin associated with the outcome of disease in patients with peripheral chondrosarcoma of the pelvis? (3) Does the histologic grade as determined with a preoperative biopsy correlate with the final grade after resection? (4) What are surgical complications in these patients?
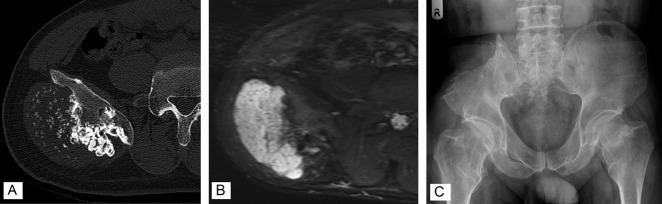
Methods: We retrospectively reviewed records from three international collaborating hospitals. Between 1983 and 2017, we resected 262 pelvic chondrosarcomas of all types. After reviewing the pathologic reports of these patients, we included 52 patients with peripheral chondrosarcomas of the pelvis who had an osteochondroma-like lesion at the base of the tumor and a cartilage cap with malignant cells in resected specimens. To be eligible for this study, a patient had to have a minimum of 1 year of follow-up. Two patients were excluded because they had less than 1 year of follow-up, leaving 50 patients for inclusion in this study. The median follow-up duration was 7.0 years (interquartile range 2.1-10 years). The median age was 37 years (IQR 29-54 years). The ilium was the most frequently affected bone (in 36 of 50 patients; 72%). The histologic status of the surgical margin was defined as microscopically positive (0 mm), negative < 1 mm, or negative ≥ 1 mm. Thirteen of the 50 patients (26%) had local recurrence. Seven of 34 patients had Grade I tumors, five of 13 had Grade II tumors, and one of three had a Grade III tumor. Nine of 16 patients had multiple local recurrences. Two patients with Grade I tumors and two with Grade II tumors died because of pressure effects caused by local recurrence.
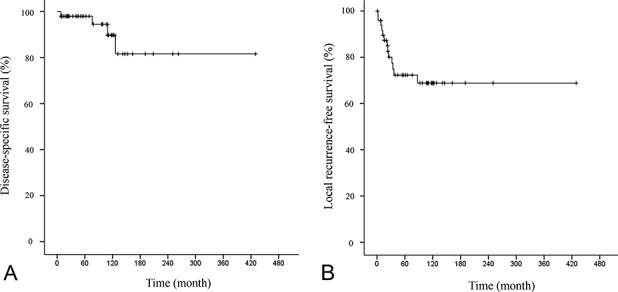
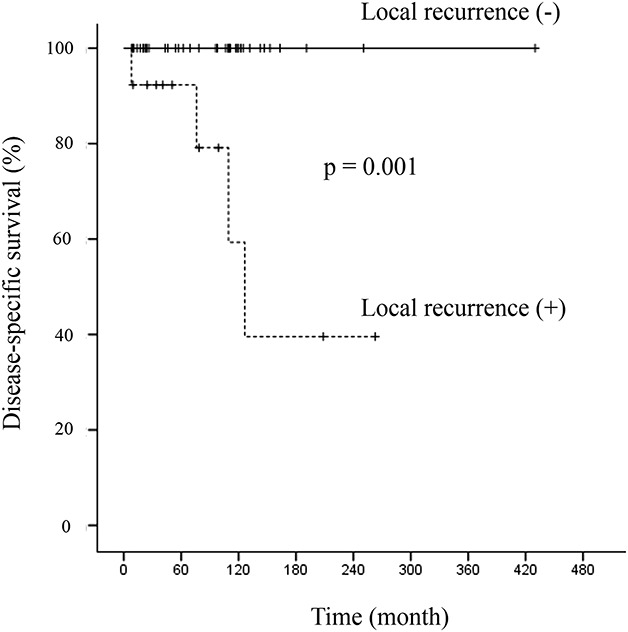
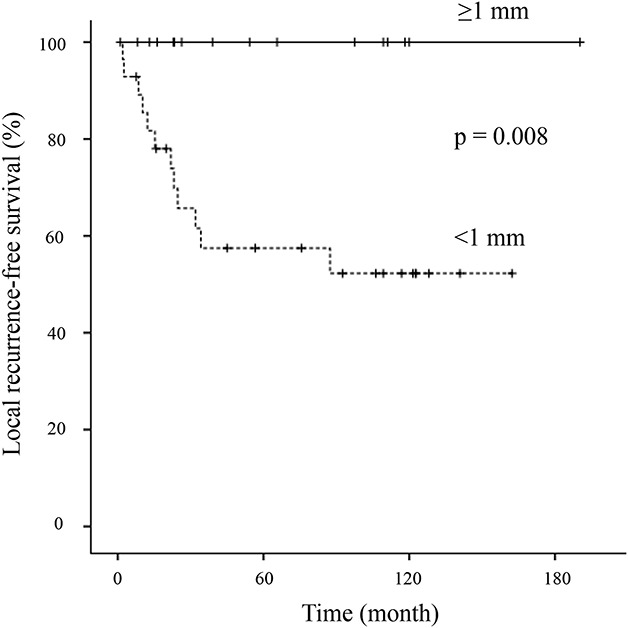
Results: The 10-year disease-specific and local recurrence-free survival rates were 90% (95% confidence interval, 70-97) and 69% (95% CI, 52-81), respectively. A surgical margin ≥ 1 mm (n = 16) was associated with a better local recurrence-free survival rate than a surgical margin < 1 mm (n = 17) or 0 mm (n = 11) (10-year local recurrence-free survival: resection margin ≥ 1 mm = 100% versus < 1 mm = 52% [95% CI, 31 to 70]; p = 0.008). No patients with a surgical margin ≥ 1 mm had local recurrence, metastasis, or disease-related death, irrespective of tumor grade. Patients with local recurrence (n = 13) showed worse disease-specific survival than those without local recurrence (n = 37) (10-year disease-specific survival: local recurrence [+] = 59% [95% CI, 16 to 86] versus local recurrence [-] = 100%; p=0.001]). The preoperative biopsy results correctly determined the tumor grade in 15 of 41 patients (37%). The most frequent complication after surgery was local recurrence (13 of 50 patients, 26%). Deep infection was the most frequent nononcologic complication (four patients).
Conclusions: We found a high local recurrence rate after surgical treatment of a peripheral pelvic chondrosarcoma, which was related to the width of the surgical margin. These local recurrences led to inoperable recurrent tumors and death. The tumor grade as determined by preoperative biopsy was inaccurate in 2/3 of patients compared with the final histologic assessment. Therefore, we believe every attempt should be made to achieve a negative margin during the initial resection to lessen the likelihood of local recurrence of peripheral chondrosarcoma of the pelvis of all grades. A margin of 1 mm or more appeared to be sufficient in these patients.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR® Tumor Board: Is the Width of a Surgical Margin Associated with the Outcome of Disease in Patients with Peripheral Chondrosarcoma of the Pelvis? A Multicenter Study.Clin Orthop Relat Res. 2019 Nov;477(11):2429-2431. doi: 10.1097/CORR.0000000000000983. Clin Orthop Relat Res. 2019. PMID: 31567581 Free PMC article. No abstract available.
-
CORR Insights®: Is the Width of a Surgical Margin Associated with the Outcome of Disease in Patients with Peripheral Chondrosarcoma of the Pelvis? A Multicenter Study.Clin Orthop Relat Res. 2019 Nov;477(11):2441-2442. doi: 10.1097/CORR.0000000000000982. Clin Orthop Relat Res. 2019. PMID: 31567582 Free PMC article. No abstract available.
Similar articles
-
Can the Cartilaginous Thickness Determine the Risk of Malignancy in Pelvic Cartilaginous Tumors, and How Accurate is the Preoperative Biopsy of These Tumors?Clin Orthop Relat Res. 2024 Jun 1;482(6):1006-1016. doi: 10.1097/CORR.0000000000003065. Epub 2024 Apr 9. Clin Orthop Relat Res. 2024. PMID: 38901841 Free PMC article.
-
Locally recurrent chondrosarcoma of the pelvis and limbs can only be controlled by wide local excision.Bone Joint J. 2019 Mar;101-B(3):266-271. doi: 10.1302/0301-620X.101B3.BJJ-2018-0881.R1. Bone Joint J. 2019. PMID: 30813783
-
Pelvic chondrosarcomas: surgical treatment options.Orthop Traumatol Surg Res. 2009 Oct;95(6):393-401. doi: 10.1016/j.otsr.2009.05.004. Epub 2009 Oct 3. Orthop Traumatol Surg Res. 2009. PMID: 19801212
-
Chondrosarcoma of the pelvis. A review of sixty-four cases.J Bone Joint Surg Am. 2001 Nov;83(11):1630-42. J Bone Joint Surg Am. 2001. PMID: 11701784 Review.
-
Intralesional treatment versus wide resection for central low-grade chondrosarcoma of the long bones.Cochrane Database Syst Rev. 2019 Mar 7;3(3):CD010778. doi: 10.1002/14651858.CD010778.pub2. Cochrane Database Syst Rev. 2019. PMID: 30845364 Free PMC article.
Cited by
-
CORR Insights®: Is the Width of a Surgical Margin Associated with the Outcome of Disease in Patients with Peripheral Chondrosarcoma of the Pelvis? A Multicenter Study.Clin Orthop Relat Res. 2019 Nov;477(11):2441-2442. doi: 10.1097/CORR.0000000000000982. Clin Orthop Relat Res. 2019. PMID: 31567582 Free PMC article. No abstract available.
-
Chondrosarcoma: A Clinical Review.J Clin Med. 2023 Mar 26;12(7):2506. doi: 10.3390/jcm12072506. J Clin Med. 2023. PMID: 37048590 Free PMC article. Review.
-
The clinical outcomes and prognostic factors of dedifferentiated central chondrosarcoma in extremities.J Orthop Surg Res. 2024 Oct 3;19(1):621. doi: 10.1186/s13018-024-05098-9. J Orthop Surg Res. 2024. PMID: 39363319 Free PMC article.
-
A Radiological Scoring System for Differentiation between Enchondroma and Chondrosarcoma.Cancers (Basel). 2021 Jul 16;13(14):3558. doi: 10.3390/cancers13143558. Cancers (Basel). 2021. PMID: 34298772 Free PMC article.
-
Primary Chondrosarcoma of the Right Fourth Rib Resected at the Marginal Margin: A Case Report.Cureus. 2023 Dec 28;15(12):e51251. doi: 10.7759/cureus.51251. eCollection 2023 Dec. Cureus. 2023. PMID: 38288168 Free PMC article.
References
-
- Ahmed AR, Tan TS, Unni KK, Collins MS, Wenger DE, Sim FH. Secondary chondrosarcoma in osteochondroma: report of 107 patients. Clin Orthop Relat Res . 2003;411:193-206. - PubMed
-
- Bus MP, Campanacci DA, Albergo JI, Leithner A, van de Sande MA, Gaston CL, Caff G, Mettelsiefen J, Capanna R, Tunn PU, Jeys LM, Dijkstra PD. Conventional primary central chondrosarcoma of the pelvis: prognostic factors and outcome of surgical treatment in 162 patients. J Bone Joint Surg Am . 2018;21:316-325. - PubMed
-
- Casali PG, Bielack S, Abecassis N, Aro HT, Bauer S, Biagini R, Bonvalot S, Boukovinas I, Bovee JV, Brennan B, Brodowicz T, Broto JM, Brugières L, Buonadonna A, De Álava E, Dei Tos AP, Del Muro XG, Dileo P, Dhooge C, Eriksson M, Fagioli F, Fedenko A, Ferraresi V, Ferrari A, Ferrari S, Frezza AM, Gaspar N, Gasperoni S, Gelderblom H, Gil T, Grignani G, Gronchi A, Haas RL, Hassan B, Hecker-Nolting S, Hohenberger P, Issels R, Joensuu H, Jones RL, Judson I, Jutte P, Kaal S, Kager L, Kasper B, Kopeckova K, Krákorová DA, Ladenstein R, Le Cesne A, Lugowska I, Merimsky O, Montemurro M, Morland B, Pantaleo MA, Piana R, Picci P, Piperno-Neumann S, Pousa AL, Reichardt P, Robinson MH, Rutkowski P, Safwat AA, Schöffski P, Sleijfer S, Stacchiotti S, Strauss SJ, Sundby Hall K, Unk M, Van Coevorden F, van der Graaf WT, Whelan J, Wardelmann E, Zaikova O, Blay JY; ESMO Guidelines Committee, PaedCan and ERN EURACAN. Bone sarcomas: ESMO-PaedCan-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;1:29:iv79-iv95. - PubMed
-
- Deloin X, Dumaine V, Biau D, Karoubi M, Babinet A, Tomeno B, Anract P. Pelvic chondrosarcomas: surgical treatment options. Orthop Traumatol Surg Res . 2009;95:393-401. - PubMed
-
- Donati D, El Ghoneimy A, Bertoni F, Di Bella C, Mercuri M. Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br. 2005;87:1527-1530. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
