

Examining ODD/ADHD Symptom Dimensions as Predictors of Social, Emotional, and Academic Trajectories in Middle Childhood
- PMID: 31454272
- PMCID: PMC7044073
- DOI: 10.1080/15374416.2019.1644645
Examining ODD/ADHD Symptom Dimensions as Predictors of Social, Emotional, and Academic Trajectories in Middle Childhood
Abstract
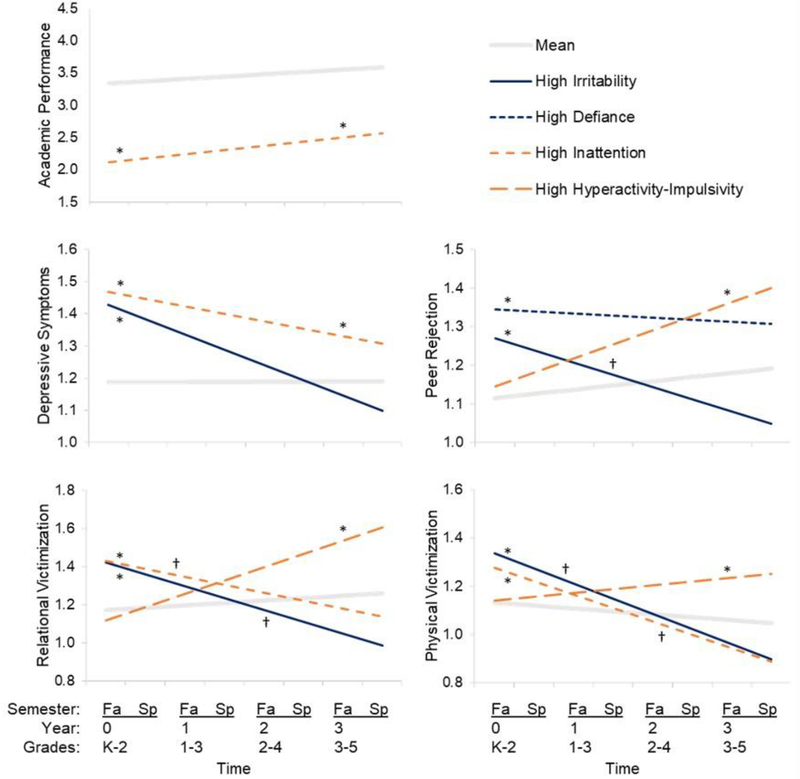
The goal of this article is to investigate the symptom dimensions of oppositional defiant disorder (ODD; irritability, defiance) and attention deficit/hyperactivity disorder (ADHD; inattention, hyperactivity-impulsivity) as predictors of academic performance, depressive symptoms, and peer functioning in middle childhood. Children (N = 346; 51% female) were assessed via teacher-report on measures of ODD/ADHD symptoms at baseline (Grades K-2) and academic performance, depressive symptoms, peer rejection, and victimization on 7 occasions over 4 school years (K-2 through 3-5). Self-report and grade point average data collected in Grades 3-5 served as converging outcome measures. Latent growth curve and multiple regression models were estimated using a hierarchical/sensitivity approach to assess robustness and specificity of effects. Irritability predicted higher baseline depressive symptoms, peer rejection, and victimization, whereas defiance predicted higher baseline peer rejection; however, none of these ODD-related effects persisted 3 years later to Grades 3-5. In contrast, inattention predicted persistently poorer academic performance, persistently higher depressive symptoms, and higher baseline victimization; hyperactivity-impulsivity predicted subsequent peer rejection and victimization in Grades 3-5. In converging models, only inattention emerged as a robust predictor of 3-year outcomes (viz., grade point average, depressive symptoms, peer rejection, and relational victimization). Broadly, ODD dimensions-particularly irritability-may be linked to acute disturbances in social-emotional functioning in school-age children, whereas ADHD dimensions may predict more persistent patterns of peer, affective, and academic problems. By examining all 4 ODD/ADHD symptom dimensions simultaneously, the present analyses offer clarity and specificity regarding which dimensions affect what outcomes, and when. Findings underscore the importance of multidimensional approaches to research, assessment, and intervention.
Figures
References
-
- Achenbach TM, & Rescorla LA (2001). Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.
-
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, D.C: American Psychiatric Association.
-
- Angold A, Costello EJ, Messer SC, & Pickles A (1995). Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. International Journal of Methods in Psychiatric Research, 5, 237–249.
-
- Axelson D, Findling RL, Fristad MA, Kowatch RA, Youngstrom EA, Horwitz SM, ... & Gill MK (2012). Examining the proposed disruptive mood dysregulation disorder diagnosis in children in the Longitudinal Assessment of Manic Symptoms study. The Journal of Clinical Psychiatry, 73(10), 1342–1350 - PMC - PubMed
-
- Bagwell CL, Molina BSG, Pelham WE, & Hoza B (2001). Attention-deficit hyperactivity disorder and problems in peer relations: Predictions from childhood to adolescence. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 1285–1292. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical