

Impact on child acute malnutrition of integrating a preventive nutrition package into facility-based screening for acute malnutrition during well-baby consultation: A cluster-randomized controlled trial in Burkina Faso
- PMID: 31454347
- PMCID: PMC6711504
- DOI: 10.1371/journal.pmed.1002877
Impact on child acute malnutrition of integrating a preventive nutrition package into facility-based screening for acute malnutrition during well-baby consultation: A cluster-randomized controlled trial in Burkina Faso
Abstract
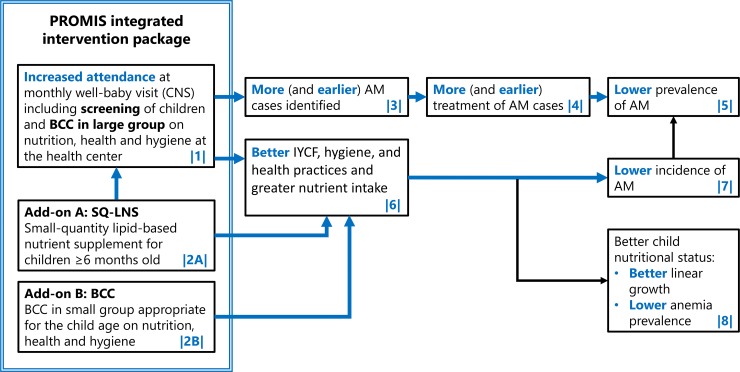
Background: Community management of acute malnutrition (CMAM) is a highly efficacious approach for treating acute malnutrition (AM) in children who would otherwise be at significantly increased risk of mortality. In program settings, however, CMAM's effectiveness is limited because of low screening coverage of AM, in part because of the lack of perceived benefits for caregivers. In Burkina Faso, monthly screening for AM of children <2 years of age is conducted during well-baby consultations (consultation du nourrisson sain [CNS]) at health centers. We hypothesized that the integration of a preventive package including age-appropriate behavior change communication (BCC) on nutrition, health, and hygiene practices and a monthly supply of small-quantity lipid-based nutrient supplements (SQ-LNSs) to the monthly screening would increase AM screening and treatment coverage and decrease the incidence and prevalence of AM.
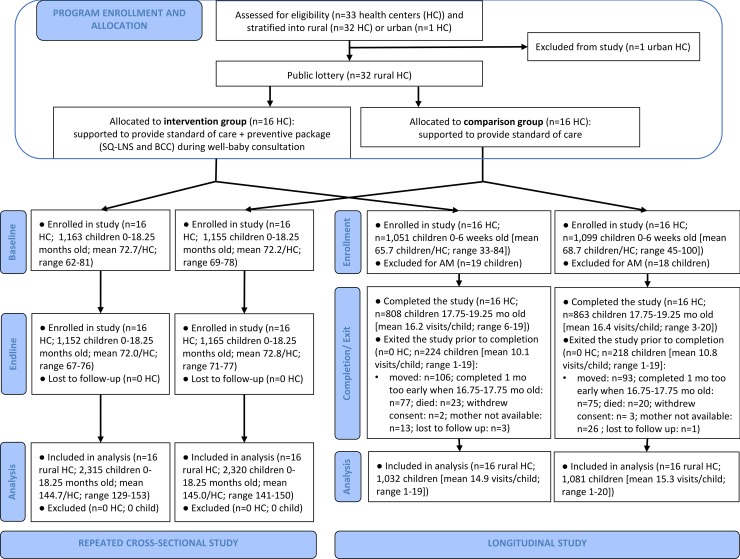
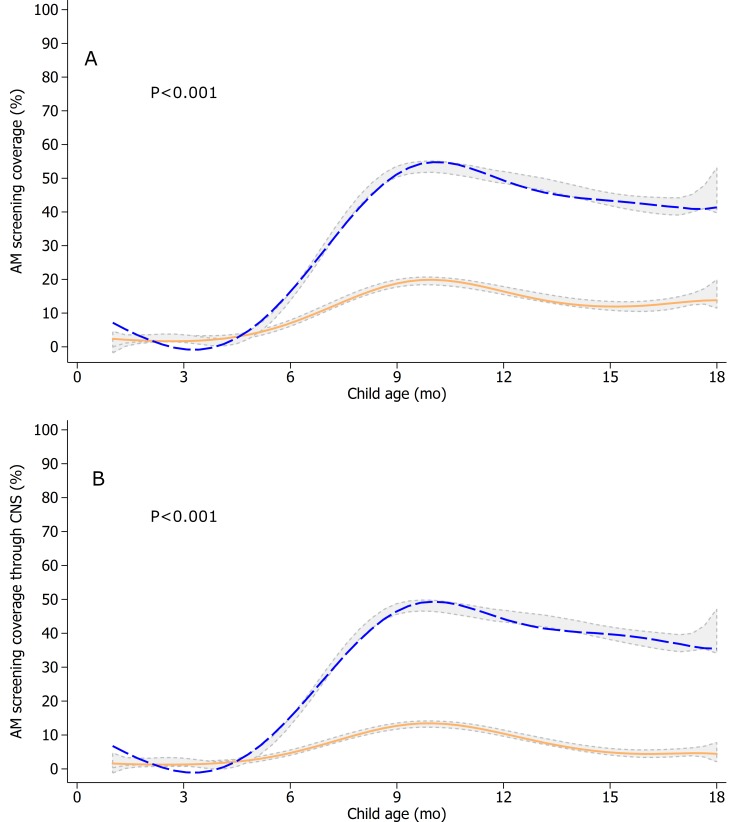
Methods and findings: We used a cluster-randomized controlled trial and allocated 16 health centers to the intervention group and 16 to a comparison group. Both groups had access to standard CMAM and CNS services; caregivers in the intervention group also received age-appropriate monthly BCC and SQ-LNS for children >6 months of age. We used two study designs: (1) a repeated cross-sectional study of children 0-17 months old (n = 2,318 and 2,317 at baseline and endline 2 years later) to assess impacts on AM screening coverage, treatment coverage, and prevalence; (2) a longitudinal study of 2,113 children enrolled soon after birth and followed up monthly for 18 months to assess impacts on AM screening coverage, treatment coverage, and incidence. Data were analyzed as intent to treat. Level of significance for primary outcomes was α = 0.016 after adjustment for multiple testing. Children's average age was 8.8 ± 4.9 months in the intervention group and 8.9 ± 5.0 months in the comparison group at baseline and, respectively, 0.66 ± 0.32 and 0.67 ± 0.33 months at enrollment in the longitudinal study. Relative to the comparison group, the intervention group had significantly higher monthly AM screening coverage (cross-sectional study: +18 percentage points [pp], 95% CI 10-26, P < 0.001; longitudinal study: +23 pp, 95% CI 17-29, P < 0.001). There were no impacts on either AM treatment coverage (cross-sectional study: +8.0 pp, 95% CI 0.09-16, P = 0.047; longitudinal study: +7.7 pp, 95% CI -1.2 to 17, P = 0.090), AM incidence (longitudinal study: incidence rate ratio = 0.98, 95% CI 0.75-1.3, P = 0.88), or AM prevalence (cross-sectional study: -0.46 pp, 95% CI -4.4 to 3.5, P = 0.82). A study limitation is the referral of AM cases (for ethical reasons) by study enumerators as part of the monthly measurement in the longitudinal study that may have attenuated the detectable impact on AM treatment coverage.
Conclusions: Adding a preventive package to CMAM delivered at health facilities in Burkina Faso increased participation in monthly AM screening, thus overcoming a major impediment to CMAM effectiveness. The lack of impact on AM treatment coverage and on AM prevalence and incidence calls for research to address the remaining barriers to uptake of preventive and treatment services at the health center and to identify and test complementary approaches to bring integrated preventive and CMAM services closer to the community while ensuring high-quality implementation and service delivery.
Trial registration: ClinicalTrials.gov NCT02245152.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- UNICEF, WHO, The World Bank group. Levels and trends in child malnutrition. Joint child malnutrition estimates 2017. edition [Internet]. 2017. Available from: https://www.who.int/nutgrowthdb/jme_brochoure2017.pdf. [cited 2019 March 12].
-
- World Health Organization, World Food Programme, United Nations System Standing Committee on Nutrition, United Nations Children’s Fund. Community-based management of severe acute malnutrition: A joint Statement by the World Health Organization, the World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children's Fund. Geneva: World Health Organization; 2007.
-
- World Health Organization. Technical note: Supplementary foods for the management of moderate acute malnutrition in infants and children 6–59 months of age. World Health Organization: 2012. 10.1227/00006123-199112000-00028 - DOI
-
- International Food Policy Research Institute. Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030. Washington, DC: 2016.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
