

Effect of delayed misoprostol dosing interval for induction of labor: a retrospective study
- PMID: 31455215
- PMCID: PMC6712846
- DOI: 10.1186/s12884-019-2454-9
Effect of delayed misoprostol dosing interval for induction of labor: a retrospective study
Abstract
Background: Induction of labor occurs in greater than 22% of all pregnancies in the United States. Previous studies have shown that misoprostol is more effective for induction than oxytocin or dinoprostone alone. The World Health Organization recommends vaginal misoprostol 25mcg every 6 hours and the American Congress of Obstetricians and Gynecologists recommends 25mcg vaginal misoprostol every three to 6 hours. Although route of administration and dosage of misoprostol has been extensively studied, little is known about the optimal dosing interval of vaginal misoprostol.
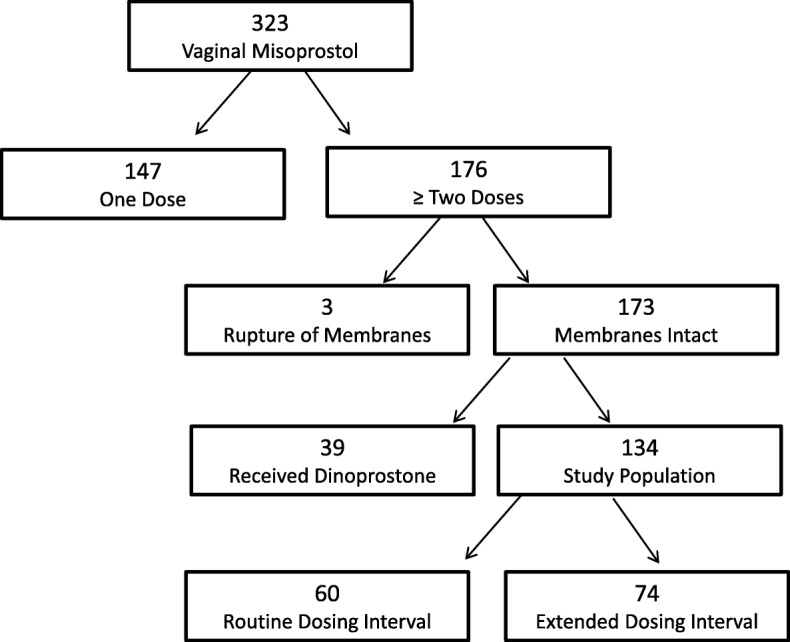
Methods: The primary objective of this study is to determine the effect of delayed vaginal misoprostol dosing, defined as any interval longer than 4.5 h, on time to vaginal delivery. Our hypothesis is that the routine dosing interval of 4 hours shortens times to vaginal delivery compared to delayed dosing, even when adjusted for the time of delay. Secondary objectives include the effect of delayed vaginal misoprostol dosing on cesarean section rate, operative vaginal delivery rate, maternal outcomes, and neonatal outcomes. We conducted a retrospective chart review of 323 inductions of labor at one academic institution. The primary outcome was the proportion of patients who achieved a vaginal delivery within 24 h. The group who received all doses of misoprostol within a 4.5 h dosing window (Routine Dosing Interval Group) was compared with the group who had any dosing deviation (Delayed Dosing Interval Group).
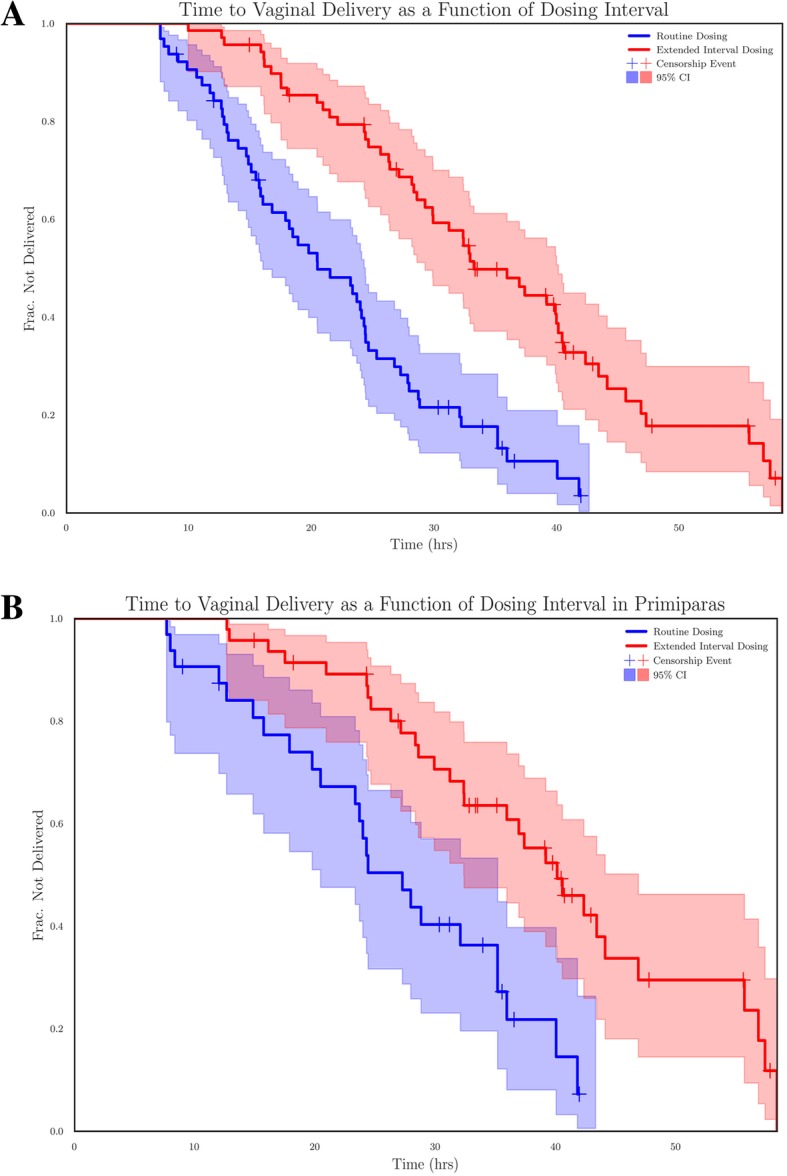
Results: Of 133 included patients, 64 subjects received routine interval dosing and 69 subjects received delayed interval dosing. The vaginal delivery rates within 24 h were 56% (36/64) and 20% (14/69), respectively (P < 10- 4). Spontaneous vaginal delivery rates were 86% (55/64) vs. 75% (52/69), respectively (P = .13). Kaplan Meier curves demonstrated statistically significant difference in time to vaginal delivery between groups, with a Cox Proportional Hazard ratio for routine dosing interval of 1.73 (P < 10- 5) unadjusted and 1.34 (P = .01) when adjusted for dosing delay.
Conclusions: This retrospective study demonstrates a significant increase in delay-adjusted time to vaginal delivery when doses of vaginal misoprostol are delayed past 4.5 h.
Keywords: Cesarean section; Induction; Misoprostol; Multiparty; Nulliparity; Vaginal delivery.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Induction of labor using one dose vs multiple doses of misoprostol: a randomized controlled trial.Am J Obstet Gynecol. 2018 Jun;218(6):614.e1-614.e8. doi: 10.1016/j.ajog.2018.03.034. Epub 2018 Mar 31. Am J Obstet Gynecol. 2018. PMID: 29614276 Clinical Trial.
-
A comparison of differing dosing regimens of vaginally administered misoprostol for preinduction cervical ripening and labor induction.Am J Obstet Gynecol. 1996 Jul;175(1):158-64. doi: 10.1016/s0002-9378(96)70267-3. Am J Obstet Gynecol. 1996. PMID: 8694043 Clinical Trial.
-
Labor induction with misoprostol vaginal insert compared with dinoprostone vaginal insert.Acta Obstet Gynecol Scand. 2019 Oct;98(10):1268-1273. doi: 10.1111/aogs.13667. Epub 2019 Jun 18. Acta Obstet Gynecol Scand. 2019. PMID: 31140585
-
Balancing the efficacy and safety of misoprostol: a meta-analysis comparing 25 versus 50 micrograms of intravaginal misoprostol for the induction of labour.BJOG. 2015 Mar;122(4):468-76. doi: 10.1111/1471-0528.12935. Epub 2014 Jul 3. BJOG. 2015. PMID: 24989790 Review.
-
Foley catheter versus vaginal misoprostol: randomized controlled trial (PROBAAT-M study) and systematic review and meta-analysis of literature.Am J Perinatol. 2014 Feb;31(2):145-56. doi: 10.1055/s-0033-1341573. Epub 2013 Apr 5. Am J Perinatol. 2014. PMID: 23564065 Clinical Trial.
Cited by
-
Maternal and fetal outcomes in women undergoing induction of labor with low dose vaginal misoprostol.Pak J Med Sci. 2023 Sep-Oct;39(5):1307-1311. doi: 10.12669/pjms.39.5.7072. Pak J Med Sci. 2023. PMID: 37680840 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
