

Comparative Genomics of Antibiotic-Resistant Uropathogens Implicates Three Routes for Recurrence of Urinary Tract Infections
- PMID: 31455657
- PMCID: PMC6712402
- DOI: 10.1128/mBio.01977-19
Comparative Genomics of Antibiotic-Resistant Uropathogens Implicates Three Routes for Recurrence of Urinary Tract Infections
Abstract
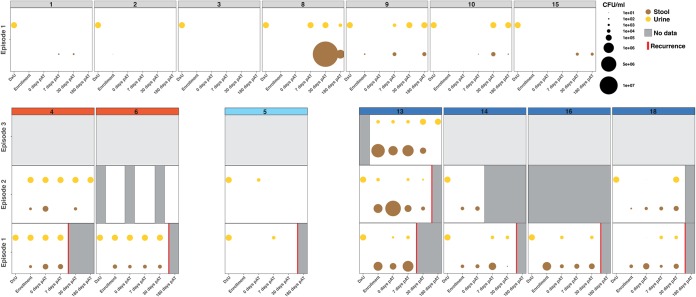
The rise of antimicrobial resistance in uropathogens has complicated the management of urinary tract infections (UTIs), particularly in patients who are afflicted by recurrent episodes of UTIs. Antimicrobial-resistant (AR) uropathogens persistently colonizing individuals at asymptomatic time points have been implicated in the pathophysiology of UTIs. The dynamics of uropathogen persistence following the resolution of symptomatic disease are, however, mostly unclear. To further our understanding, we determined longitudinal AR uropathogen carriage and clonal persistence of uropathogenic Escherichia coli, Proteus mirabilis, and Klebsiella pneumoniae isolates in the intestinal and urinary tracts of patients affected by recurrent and nonrecurrent UTIs. Clonal tracking of isolates in consecutively collected urine and fecal specimens indicated repeated transmission of uropathogens between the urinary tract and their intestinal reservoir. Our results further implicate three independent routes of recurrence of UTIs: (i) following an intestinal bloom of uropathogenic bacteria and subsequent bladder colonization, (ii) reinfection of the urinary tract from an external source, and (iii) bacterial persistence within the urinary tract. Taken together, our observation of clonal persistence following UTIs and uropathogen transmission between the intestinal and urinary tracts warrants further investigations into the connection between the intestinal microbiome and recurrent UTIs.IMPORTANCE The increasing antimicrobial resistance of uropathogens is challenging the continued efficacy of empiric antibiotic therapy for UTIs, which are among the most frequent bacterial infections worldwide. It has been suggested that drug-resistant uropathogens could persist in the intestine after the resolution of UTI and cause recurrences following periurethral contamination. A better understanding of the transmission dynamics between the intestinal and urinary tracts, combined with phenotypic characterization of the uropathogen populations in both habitats, could inform prudent therapies designed to overcome the rising resistance of uropathogens. Here, we integrate genomic surveillance with clinical microbiology to show that drug-resistant clones persist within and are readily transmitted between the intestinal and urinary tracts of patients affected by recurrent and nonrecurrent UTIs. Thus, our results advocate for understanding persistent intestinal uropathogen colonization as part of the pathophysiology of UTIs, particularly in patients affected by recurrent episodes of symptomatic disease.
Keywords: antibiotic resistance; clonal tracking; comparative genomics; recurrence; urinary tract infection.
Copyright © 2019 Thänert et al.
Figures



References
-
- Rubin RH, Shapiro ED, Andriole VT, Davis RJ, Stamm WE. 1992. Evaluation of new anti-infective drugs for the treatment of urinary tract infection. Infectious Diseases Society of America and the Food and Drug Administration. Clin Infect Dis 15(Suppl 1):S216–S227. doi: 10.1093/clind/15.Supplement_1.S216. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
