

Death after hematopoietic stem cell transplantation: changes over calendar year time, infections and associated factors
- PMID: 31455899
- PMCID: PMC6957465
- DOI: 10.1038/s41409-019-0624-z
Death after hematopoietic stem cell transplantation: changes over calendar year time, infections and associated factors
Abstract
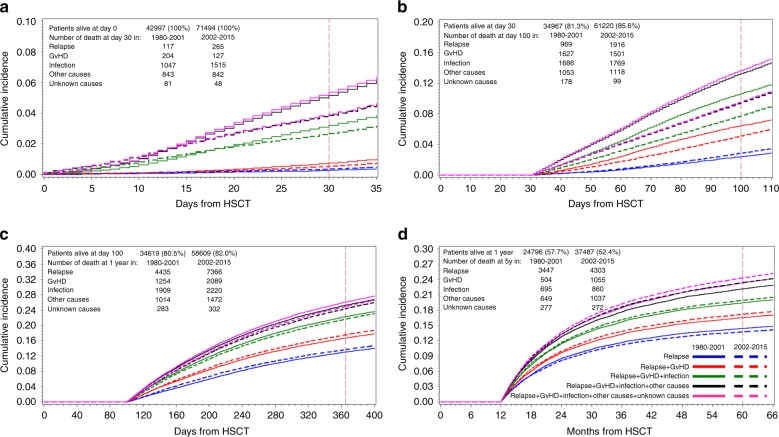
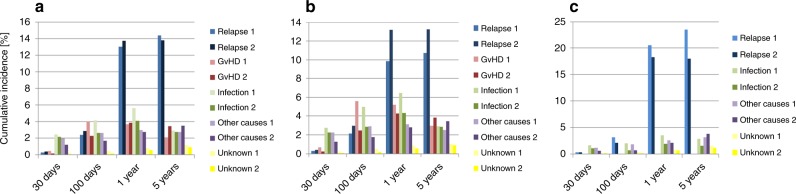
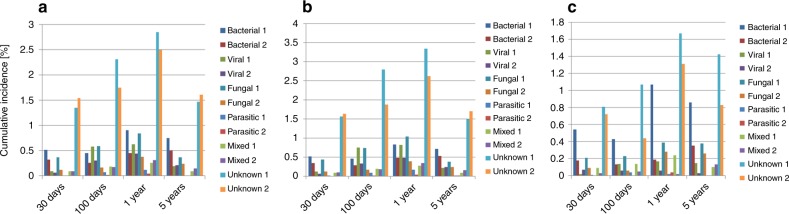
Information on incidence, and factors associated with mortality is a prerequisite to improve outcome after hematopoietic stem cell transplantation (HSCT). Therefore, 55'668 deaths in 114'491 patients with HSCT (83.7% allogeneic) for leukemia were investigated in a landmark analysis for causes of death at day 30 (very early), day 100 (early), at 1 year (intermediate) and at 5 years (late). Mortality from all causes decreased from cohort 1 (1980-2001) to cohort 2 (2002-2015) in all post-transplant phases after autologous HSCT. After allogeneic HSCT, mortality from infections, GVHD, and toxicity decreased up to 1 year, increased at 5 years; deaths from relapse increased in all post-transplant phases. Infections of unknown origin were the main cause of infectious deaths. Lethal bacterial and fungal infections decreased from cohort 1 to cohort 2, not unknown or mixed infections. Infectious deaths were associated with patient-, disease-, donor type, stem cell source, center, and country- related factors. Their impact varied over the post-transplant phases. Transplant centres have successfully managed to reduce death after HSCT in the early and intermediate post-transplant phases, and have identified risk factors. Late post-transplant care could be improved by focus on groups at risk and better identification of infections of "unknown origin".
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Gratwohl A, Brand R, Frassoni F, Rocha V, Niederwieser D, Reusser P, et al. Cause of death after allogeneic haematopoietic stem cell transplantation (HSCT) in early leukaemias: an EBMT analysis of lethal infectious complications and changes over calendar time. Bone Marrow Transpl. 2005;36:757–69. doi: 10.1038/sj.bmt.1705140. - DOI - PubMed
-
- Passweg JR, Baldomero H, Bader P, Bonini C, Duarte RF, Dufour C, et al. Use of haploidentical stem cell transplantation continues to increase: the 2015 European Society for Blood and Marrow Transplant activity survey report. Bone Marrow Transpl. 2017;52:811–7. doi: 10.1038/bmt.2017.34. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
