

Diabetic ketoacidosis in patients with type 2 diabetes treated with sodium glucose co-transporter 2 inhibitors versus other antihyperglycemic agents: An observational study of four US administrative claims databases
- PMID: 31456304
- PMCID: PMC6916409
- DOI: 10.1002/pds.4887
Diabetic ketoacidosis in patients with type 2 diabetes treated with sodium glucose co-transporter 2 inhibitors versus other antihyperglycemic agents: An observational study of four US administrative claims databases
Abstract
Purpose: To compare the incidence of diabetic ketoacidosis (DKA) among patients with type 2 diabetes mellitus (T2DM) who were new users of sodium glucose co-transporter 2 inhibitors (SGLT2i) versus other classes of antihyperglycemic agents (AHAs).
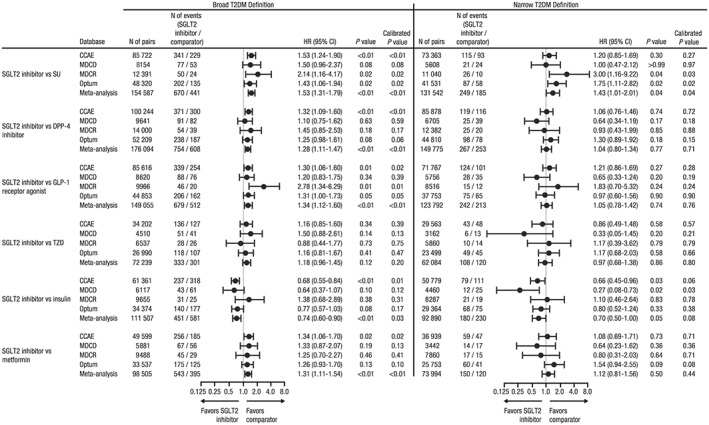
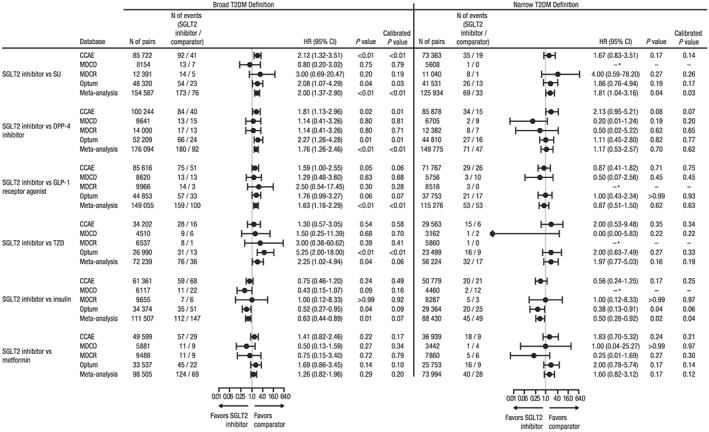
Methods: Patients were identified from four large US claims databases using broad (all T2DM patients) and narrow (intended to exclude patients with type 1 diabetes or secondary diabetes misclassified as T2DM) definitions of T2DM. New users of SGLT2i and seven groups of comparator AHAs were matched (1:1) on exposure propensity scores to adjust for imbalances in baseline covariates. Cox proportional hazards regression models, conditioned on propensity score-matched pairs, were used to estimate hazard ratios (HRs) of DKA for new users of SGLT2i versus other AHAs. When I2 <40%, a combined HR across the four databases was estimated.
Results: Using the broad definition of T2DM, new users of SGLT2i had an increased risk of DKA versus sulfonylureas (HR [95% CI]: 1.53 [1.31-1.79]), DPP-4i (1.28 [1.11-1.47]), GLP-1 receptor agonists (1.34 [1.12-1.60]), metformin (1.31 [1.11-1.54]), and insulinotropic AHAs (1.38 [1.15-1.66]). Using the narrow definition of T2DM, new users of SGLT2i had an increased risk of DKA versus sulfonylureas (1.43 [1.01-2.01]). New users of SGLT2i had a lower risk of DKA versus insulin and a similar risk as thiazolidinediones, regardless of T2DM definition.
Conclusions: Increased risk of DKA was observed for new users of SGLT2i versus several non-SGLT2i AHAs when T2DM was defined broadly. When T2DM was defined narrowly to exclude possible misclassified patients, an increased risk of DKA with SGLT2i was observed compared with sulfonylureas.
Keywords: SGLT2 inhibitor; diabetic ketoacidosis; type 2 diabetes.
© 2019 The Authors. Pharmacoepidemiology & Drug Safety Published by John Wiley & Sons Ltd.
Figures
References
-
- International Diabetes Federation . IDF Diabetes Atlas. 8th ed. Brussels, Belgium: International Diabetes Federation; 2017.
-
- Wang ZH, Kihl‐Selstam E, Eriksson JW. Ketoacidosis occurs in both Type 1 and Type 2 diabetes—a population‐based study from Northern Sweden. Diabet Med. 2008;25(7):867‐870. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
