

Surgical Management of Lower Extremity Lymphedema: A Comprehensive Review
- PMID: 31456616
- PMCID: PMC6664851
- DOI: 10.1055/s-0039-1688537
Surgical Management of Lower Extremity Lymphedema: A Comprehensive Review
Abstract
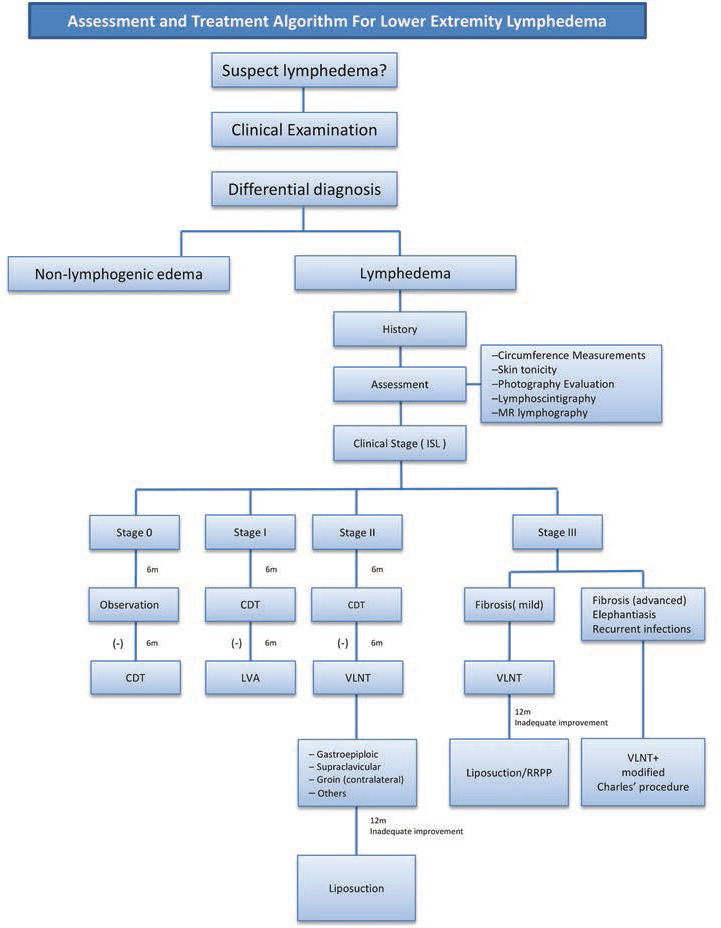
Lymphedema refers to the accumulation of protein-rich fluid in the interstitial spaces. This can occur secondary to congenital malformation of the lymphatic channels or nodes or as a result of an insult that damages appropriately formed channels and nodes. Stagnant, protein-rich lymph initiates an inflammatory response that leads to adipocyte proliferation, fibrous tissue deposition, and increased susceptibility to infections. The end result is permanent disfigurement and dermal changes. Early and accurate diagnosis is essential, since lymphedema is a chronic and progressive problem. When lymphedema affects the lower extremity, it is important to manage it in a way that preserves function and mobility. Early diagnosis also allows for a proactive rather than reactive approach to treatment and utilization of novel physiologic procedures, such as lymphovenous anastomosis and vascularized lymph node transfer. Such interventions slow down disease progression and reduce morbidity by allowing the surgeon to salvage the remaining functional lymphatic channels. When physiologic procedures fail or when faced with a delayed presentation, the addition of excisional procedures can provide a more comprehensive treatment of this debilitating disease. The aim of this article is to review the most current concepts in the surgical management of lower extremity lymphedema.
Keywords: lower extremity lymphedema; lymphedema; radical reduction in lymphedema with preservation of perforators; suction-assisted lipectomy; vascularized lymph node transfer.
Conflict of interest statement
Figures








References
-
- Shimony A, Tidhar D. Lymphedema: a comprehensive review. Ann Plast Surg. 2008;60(02):228. - PubMed
-
- International Society of Lymphology . The diagnosis and treatment of peripheral lymphedema: 2013 Consensus Document of the International Society of Lymphology. Lymphology. 2013;46(01):1–11. - PubMed
-
- Hansen K C, D'Alessandro A, Clement C C, Santambrogio L. Lymph formation, composition and circulation: a proteomics perspective. Int Immunol. 2015;27(05):219–227. - PubMed
-
- Kung T A, Champaneria M C, Maki J H, Neligan P C. Current concepts in the surgical management of lymphedema. Plast Reconstr Surg. 2017;139(04):1003e–1013e. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources