

A case of malignant melanoma after repeated recurrent dysplastic nevi
- PMID: 31462019
- PMCID: PMC6715558
- DOI: 10.7181/acfs.2019.00283
A case of malignant melanoma after repeated recurrent dysplastic nevi
Abstract
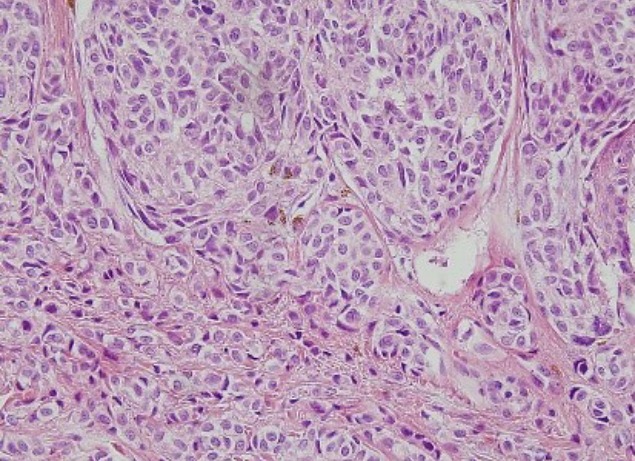
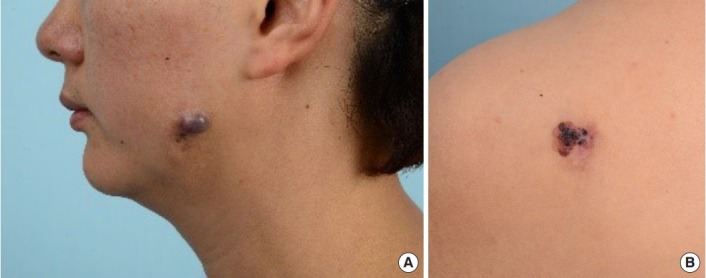
Dysplastic nevus is common and affects about 10% of the northern European-descendent population. Studies over the past several decades have identified dysplastic nevi as a risk factor for malignant melanoma. Furthermore, in rare cases, they confirmed that dysplastic nevi have progressed to melanoma. Cases in which dysplastic nevi progressed to malignant melanoma in multiple studies are not uncommon. A 35-year-old woman presented with the major symptom of multiple itchy brown nodules (2.0 cm× 1.3 cm) in the left cheek that had first appeared 20 years earlier. Complete excision was performed at the first visit; subsequent biopsy confirmed that they were dysplastic nevi. They recurred three times over 3 years at the same site, all of which were histologically diagnosed as dysplastic nevi. Five years after the final excision, a brownish nodule developed in the left cheek, with others at the left temporal region, right retroauricular region, and left shoulder at the same time. These lesions were histologically diagnosed as malignant melanoma. We experienced a case of malignant melanoma that occurred at the same site after three recurrences of dysplastic nevi. Although rare, the possibility of malignant melanoma should be considered in follow-ups in cases involving repeatedly recurrent dysplastic nevi.
Keywords: Dysplastic nevus syndrome; Melanoma; Recurrence.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures





Similar articles
-
Risk of Subsequent Cutaneous Melanoma in Moderately Dysplastic Nevi Excisionally Biopsied but With Positive Histologic Margins.JAMA Dermatol. 2018 Dec 1;154(12):1401-1408. doi: 10.1001/jamadermatol.2018.3359. JAMA Dermatol. 2018. PMID: 30304348 Free PMC article.
-
Atypical (dysplastic) nevi: outcomes of surgical excision and association with melanoma.JAMA Dermatol. 2013 Aug;149(8):928-34. doi: 10.1001/jamadermatol.2013.4440. JAMA Dermatol. 2013. PMID: 23760581
-
Atypical melanocytic nevi of the genital type with a discussion of reciprocal parenchymal-stromal interactions in the biology of neoplasia.Hum Pathol. 1998 Jan;29(1 Suppl 1):S1-24. doi: 10.1016/s0046-8177(98)80028-2. Hum Pathol. 1998. PMID: 9445124
-
The dysplastic nevus: recognition and management.Plast Reconstr Surg. 1988 Feb;81(2):280-9. doi: 10.1097/00006534-198802000-00027. Plast Reconstr Surg. 1988. PMID: 3275948 Review.
-
Dysplastic Nevi.Surg Pathol Clin. 2009 Sep;2(3):447-56. doi: 10.1016/j.path.2009.08.001. Epub 2009 Oct 29. Surg Pathol Clin. 2009. PMID: 26838531 Review.
Cited by
-
Melanoma arising from partially biopsied moderately dysplastic nevus.JAAD Case Rep. 2025 Mar 7;59:89-93. doi: 10.1016/j.jdcr.2025.01.040. eCollection 2025 May. JAAD Case Rep. 2025. PMID: 40290790 Free PMC article. No abstract available.
References
-
- Carey WP, Jr, Thompson CJ, Synnestvedt M, Guerry D 4th, Halpern A, Schultz D, et al. Dysplastic nevi as a melanoma risk factor in patients with familial melanoma. Cancer. 1994;74:3118–25. - PubMed
-
- Burden AD, Newell J, Andrew N, Kavanagh G, Connor JM, MacKie RM. Genetic and environmental influences in the development of multiple primary melanoma. Arch Dermatol. 1999;135:261–5. - PubMed
-
- Masri GD, Clark WH, Jr, Guerry D 4th, Halpern A, Thompson CJ, Elder DE. Screening and surveillance of patients at high risk for malignant melanoma result in detection of earlier disease. J Am Acad Dermatol. 1990;22(6 Pt 1):1042–8. - PubMed
-
- Weinstock MA, Barnhill RL, Rhodes AR, Brodsky GL. Reliability of the histopathologic diagnosis of melanocytic dysplasia. The Dysplastic Nevus Panel Arch Dermatol. 1997;133:953–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
