

Cardiovascular outcomes in trials of new antidiabetic drug classes: a network meta-analysis
- PMID: 31462224
- PMCID: PMC6714383
- DOI: 10.1186/s12933-019-0916-z
Cardiovascular outcomes in trials of new antidiabetic drug classes: a network meta-analysis
Abstract
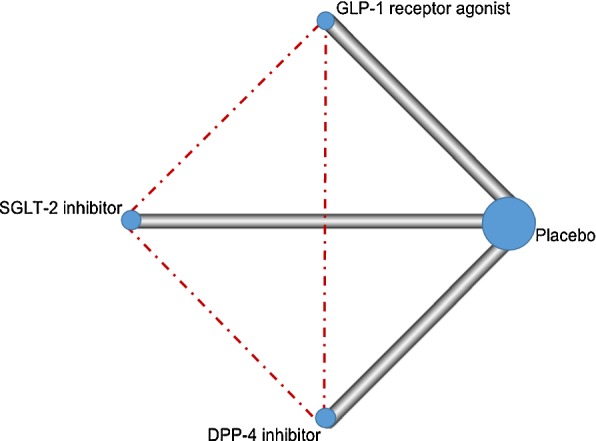
Background: Recent trials suggested that glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and sodium-glucose co-transporter-2 (SGLT-2) inhibitors reduced cardiovascular events. Comparative effectiveness of these new antidiabetic drug classes remains unclear. We therefore performed a network meta-analysis to compare the effect on cardiovascular outcomes among GLP-1 RAs, SGLT-2 and dipeptidyl peptidase-4 (DPP-4) inhibitors.
Methods: MEDLINE, EMBASE, Cochrane database, ClinicalTrials.gov, and congress proceedings from recent cardiology conferences were searched up to April 20, 2019. Cardiovascular outcome trials and renal outcome trials reporting cardiovascular outcomes on GLP-1 RAs, SGLT-2 and DPP-4 inhibitors in patients with type 2 diabetes mellitus were included. The primary outcome was major adverse cardiovascular events (MACE). Secondary outcomes were nonfatal myocardial infarction, nonfatal stroke, cardiovascular mortality, all-cause mortality, hospitalisation for heart failure (HF), and renal composite outcome. ORs and 95% CI were calculated using random-effects models.
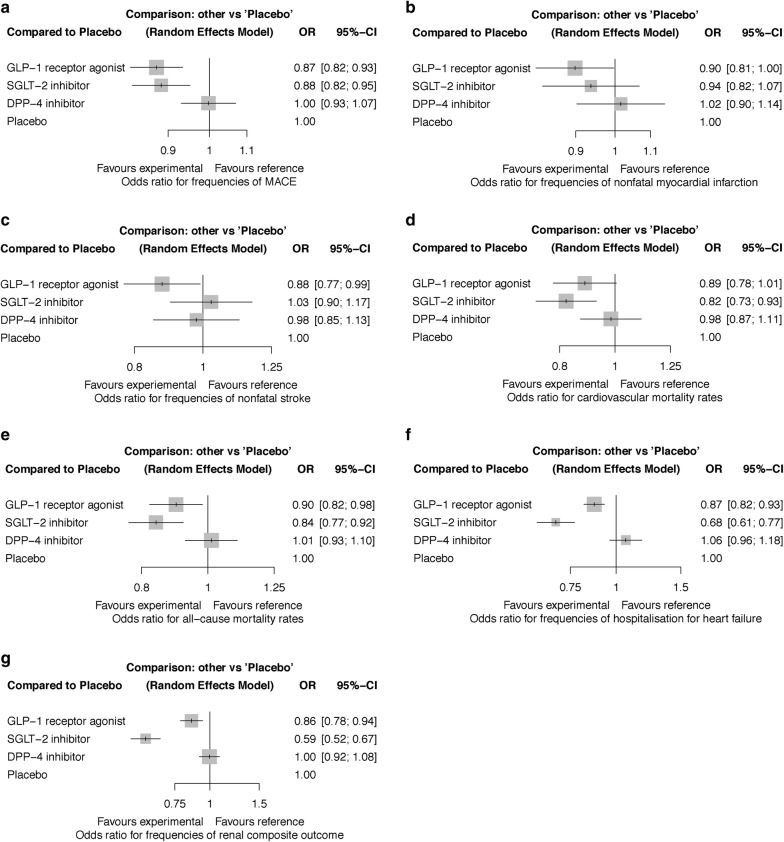
Results: Fourteen trials enrolling 121,047 patients were included. SGLT-2 inhibitors reduced cardiovascular deaths and all-cause deaths compared to placebo (OR 0.82, 95% CI 0.73-0.93 and OR 0.84, 95% CI 0.77-0.92) and DPP-4 inhibitors (OR 0.83, 95% CI 0.70-0.99 and OR 0.83, 95% CI 0.73-0.94), respectively. SGLT-2 inhibitors and GLP-1 RAs significantly reduced MACE (OR 0.88, 95% CI 0.82-0.95 and OR 0.87, 95% CI 0.82-0.93), hospitalisation for HF (OR 0.68, 95% CI 0.61-0.77 and OR 0.87, 95% CI 0.82-0.93), and renal composite outcome (OR 0.59, 95% CI 0.52-0.67 and OR 0.86, 95% CI 0.78-0.94) compared to placebo, but SGLT-2 inhibitors reduced hospitalisation for HF (OR 0.79, 95% CI 0.69-0.90) and renal composite outcome (OR 0.69, 95% CI 0.59-0.80) more than GLP-1 RAs. Only GLP-1 RAs reduced nonfatal stroke (OR 0.88, 95% CI 0.77-0.99). DPP-4 inhibitors did not lower the risk of these outcomes when compared to placebo and were associated with higher risks of MACE, hospitalisation for HF, and renal composite outcome when compared to the other two drug classes.
Conclusions: SGLT-2 inhibitors show clear superiority in reducing cardiovascular and all-cause deaths, hospitalisation for HF, and renal events among new antidiabetic drug classes. GLP-1 RAs also have cardiovascular and renal protective effects. DPP-4 inhibitors have no beneficial cardiovascular effects and are therefore inferior to the other two drug classes. SGLT-2 inhibitors should now be the preferred treatment for type 2 diabetes mellitus.
Keywords: Antidiabetic drug; Cardiovascular outcome; Network meta-analysis; Type 2 diabetes mellitus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO. Global report on diabetes. http://www.who.int/diabetes/global-report/en. Accessed 20 Nov 2018.
-
- Davies MJ, D’Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, et al. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetes Care. 2018;41(12):2669–2701. doi: 10.2337/dci18-0033. - DOI - PMC - PubMed
-
- International Diabetes Federation. IDF Clinical Practice Recommendations for managing Type 2 Diabetes in Primary Care. 2017. https://d-net.idf.org/en/library/466-managing-type-2-diabetes-in-primary.... Accessed 20 Nov 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
