

Kidney Support in Children using an Ultrafiltration Device: A Multicenter, Retrospective Study
- PMID: 31462396
- PMCID: PMC6777586
- DOI: 10.2215/CJN.03240319
Kidney Support in Children using an Ultrafiltration Device: A Multicenter, Retrospective Study
Abstract
Background and objectives: Provision of kidney replacement therapy (KRT) to manage kidney injury and volume overload in critically ill neonates and small children is technically challenging. The use of machines designed for adult-sized patients, necessitates large catheters, a high extracorporeal volume relative to patient size, and need for blood priming. The Aquadex FlexFlow System (CHF Solutions Inc., Eden Prairie, MN) is an ultrafiltration device designed for fluid removal in adults with diuretic resistant heart failure. It has an extracorporeal volume of 33 ml, which can potentially mitigate some complications seen at onset of KRT in smaller infants.
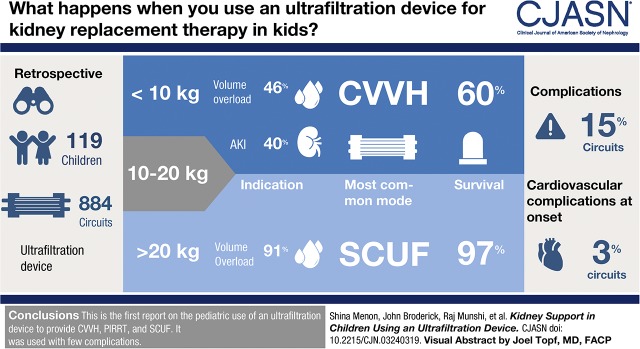
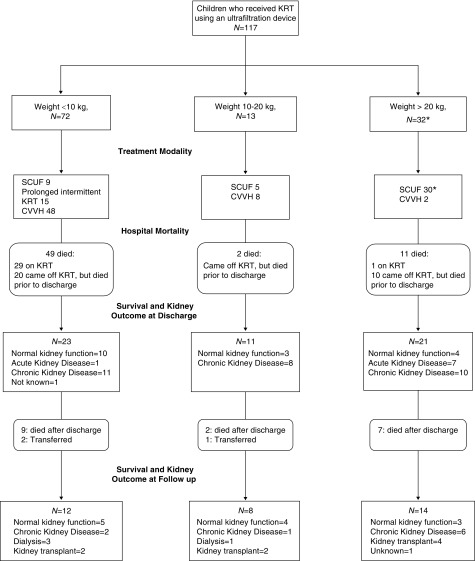
Design, setting, participants, & measurements: In this multicenter, retrospective case series of children who received KRT with an ultrafiltration device (n=119 admissions, 884 circuits), we report demographics, circuit characteristics, complications, and short- and long-term outcomes. Patients were grouped according to weight (<10, 10-20, and >20 kg), and received one of three modalities: slow continuous ultrafiltration, continuous venovenous hemofiltration (CVVH), or prolonged intermittent KRT. Our primary outcome was survival to end of KRT.
Results: Treatment patterns and outcomes varied between the groups. In patients who weighed <10 kg, the primary indication was AKI in 40%, volume overload in 46%, and ESKD in 14%. These patients primarily received CVVH (66%, n=48) and prolonged intermittent KRT (21%, n=15). In the group weighing >20 kg, volume overload was the primary indication in 91% and slow continuous ultrafiltration was the most common modality. Patients <10 kg had lower KRT survival than those >20 kg (60% versus 97%), more volume overload at onset, and received KRT for a longer duration. Cardiovascular complications at initiation were seen in 3% of treatments and none were severe. Complications during therapy were seen in 15% treatments and most were vascular access-related.
Conclusions: We report the first pediatric experience using an ultrafiltration device to provide a range of therapies, including CVVH, prolonged intermittent KRT, and slow continuous ultrafiltration. We were able to initiate KRT with minimal complications, particularly in critically ill neonates. There is an unmet need for devices specifically designed for younger patients. Having size-appropriate machines will improve the care of smaller children who require kidney support.
Keywords: acute kidney injury; acute renal failure; adult; child; chronic kidney failure; critical illness; demography; dialysis; diuretics; grassland; heart failure; hemofiltration; humans; infant; infant, newborn; kidney dialysis; kidney failure, chronic; kidney replacement therapy; renal dialysis; renal replacement therapy; retrospective studies; ultrafiltration.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Jetton JG, Boohaker LJ, Sethi SK, Wazir S, Rohatgi S, Soranno DE, Chishti AS, Woroniecki R, Mammen C, Swanson JR, Sridhar S, Wong CS, Kupferman JC, Griffin RL, Askenazi DJ; Neonatal Kidney Collaborative (NKC) : Incidence and outcomes of neonatal acute kidney injury (AWAKEN): A multicentre, multinational, observational cohort study. Lancet Child Adolesc Health 1: 184–194, 2017 - PMC - PubMed
-
- Menon S, Goldstein SL, Mottes T, Fei L, Kaddourah A, Terrell T, Arnold P, Bennett MR, Basu RK: Urinary biomarker incorporation into the renal angina index early in intensive care unit admission optimizes acute kidney injury prediction in critically ill children: A prospective cohort study. Nephrol Dial Transplant 31: 586–594, 2016 - PMC - PubMed
-
- Sutherland SM, Alexander SR: Continuous renal replacement therapy in children. Pediatr Nephrol 27: 2007–2016, 2012 - PubMed
-
- Symons JM, Brophy PD, Gregory MJ, McAfee N, Somers MJ, Bunchman TE, Goldstein SL: Continuous renal replacement therapy in children up to 10 kg. Am J Kidney Dis 41: 984–989, 2003 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
