

Lung monitoring with electrical impedance tomography: technical considerations and clinical applications
- PMID: 31463141
- PMCID: PMC6688044
- DOI: 10.21037/jtd.2019.06.27
Lung monitoring with electrical impedance tomography: technical considerations and clinical applications
Abstract
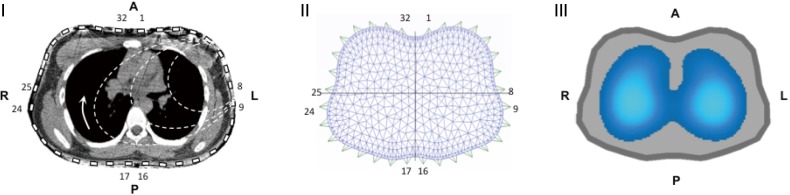
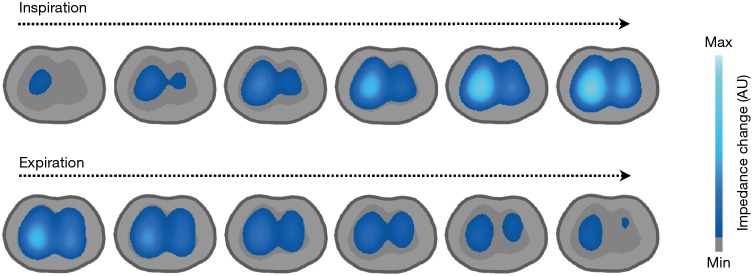
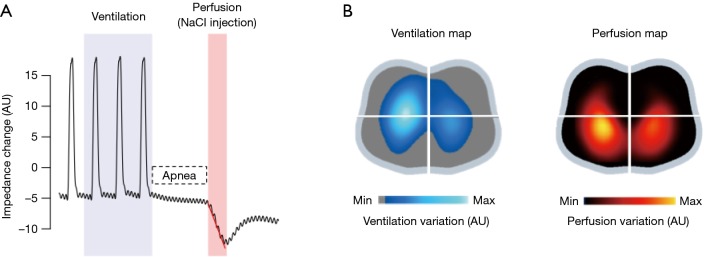
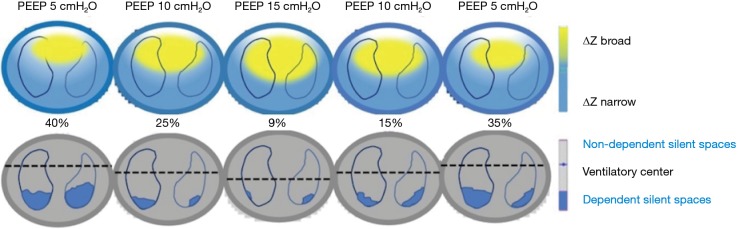
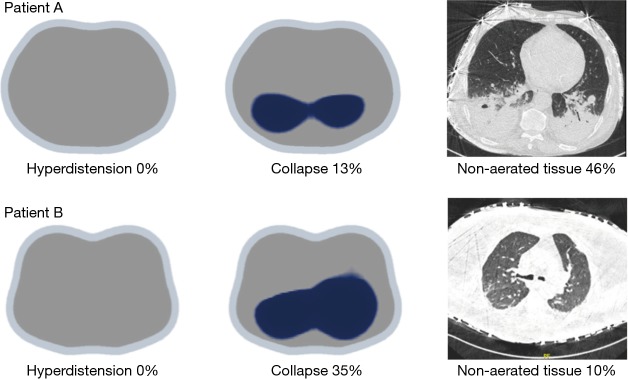
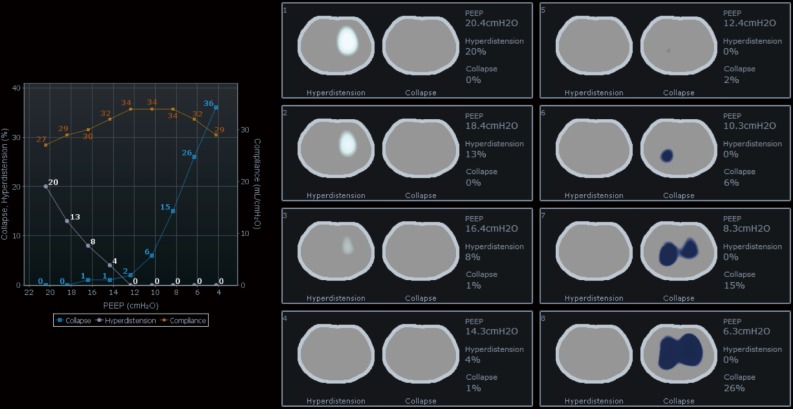
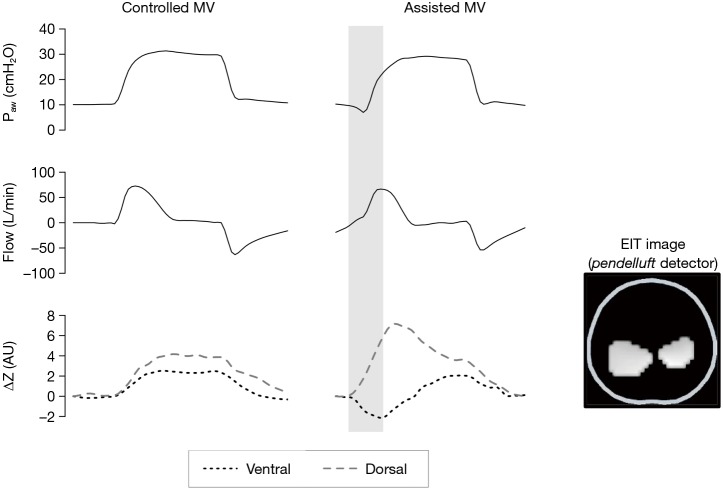
In recent years there has been substantial progress in the imaging evaluation of patients with lung disease requiring mechanical ventilatory assistance. This has been demonstrated by the inclusion of pulmonary ultrasound, positron emission tomography, electrical impedance tomography (EIT), and magnetic resonance imaging (MRI). The EIT uses electric current to evaluate the distribution of alternating current conductivity within the thoracic cavity. The advantage of the latter is that it is non-invasive, bedside radiation-free functional imaging modality for continuous monitoring of lung ventilation and perfusion. EIT can detect recruitment or derecruitment, overdistension, variation of poorly ventilated lung units (silent spaces), and pendelluft phenomenon in spontaneously breathing patients. In addition, the regional expiratory time constants have been recently explored.
Keywords: Electrical impedance tomography (EIT); acute respiratory distress syndrome (ARDS); critical care; physiologic monitoring.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources