

Determining the Association Between End-of-Life Care Resources and Patient Outcomes in Pennsylvania ICUs
- PMID: 31464767
- PMCID: PMC6791744
- DOI: 10.1097/CCM.0000000000003969
Determining the Association Between End-of-Life Care Resources and Patient Outcomes in Pennsylvania ICUs
Abstract
Objectives: As ICUs are increasingly a site of end-of-life care, many have adopted end-of-life care resources. We sought to determine the association of such resources with outcomes of ICU patients.
Design: Retrospective cohort study.
Setting: Pennsylvania ICUs.
Patients: Medicare fee-for-service beneficiaries.
Interventions: Availability of any of one hospital-based resource (palliative care consultants) or four ICU-based resources (protocol for withdrawal of life-sustaining therapy, triggers for automated palliative care consultation, protocol for family meetings, and palliative care clinicians embedded in ICU rounds).
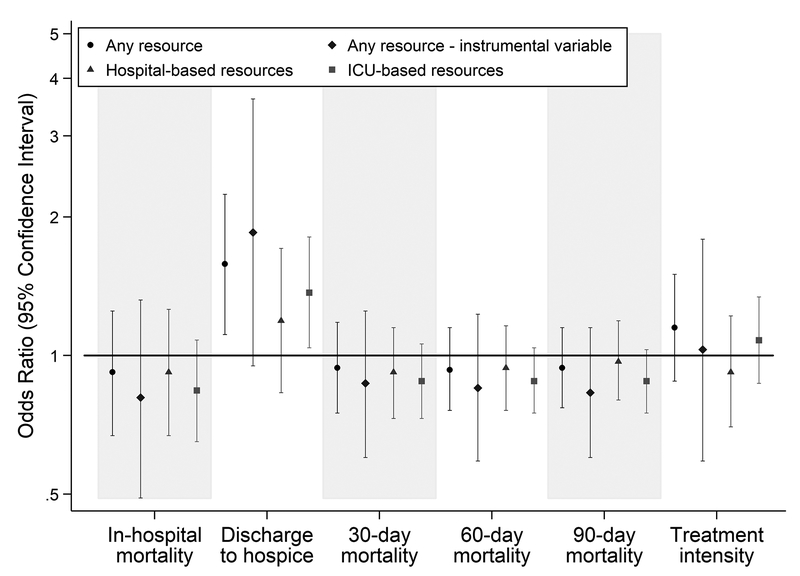
Measurements and main results: In mixed-effects regression analyses, admission to a hospital with end-of-life resources was not associated with mortality, length of stay, or treatment intensity (mechanical ventilation, hemodialysis, tracheostomy, gastrostomy, artificial nutrition, or cardiopulmonary resuscitation); however, it was associated with a higher likelihood of discharge to hospice (odds ratio, 1.58; 95% CI, 1.11-2.24), an effect that was driven by ICU-based resources (odds ratio, 1.37; 95% CI, 1.04-1.81) rather than hospital-based resources (odds ratio, 1.19; 95% CI, 0.83-1.71). Instrumental variable analysis using differential distance (defined as the additional travel distance beyond the hospital closest to a patient's home needed to reach a hospital with end-of-life resources) demonstrated that among those for whom differential distance would influence receipt of end-of-life resources, admission to a hospital with such resources was not associated with any outcome.
Conclusions: ICU-based end-of-life care resources do not appear to change mortality but are associated with increased hospice utilization. Given that this finding was not confirmed by the instrumental variable analysis, future studies should attempt to verify this finding, and identify specific resources or processes of care that impact the care of ICU patients at the end of life.
Figures
Comment in
-
The Disappearing Dichotomy Between Critical Care and Palliative Care: Integration Will Enhance Patient Outcomes.Crit Care Med. 2019 Nov;47(11):1667-1668. doi: 10.1097/CCM.0000000000003994. Crit Care Med. 2019. PMID: 31609267 No abstract available.
References
-
- Cook D, Rocker G. Dying with Dignity in the Intensive Care Unit. The New England Journal of Medicine. 2014;370(26):2506–2514. - PubMed
-
- Lustbader D, Pekmezaris R, Frankenthaler M, et al. Palliative medicine consultation impacts DNR designation and length of stay for terminal medical MICU patients. Palliative & Supportive Care. 2011;9(4):401–406. - PubMed
-
- Campbell ML, Guzman JA. Impact of a Proactive Approach to Improve End-of-Life Care in a Medical ICU. Chest. 2003;123(1):266–271. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
