

Role of Bronchoscopic Techniques in the Diagnosis of Thoracic Sarcoidosis
- PMID: 31466346
- PMCID: PMC6780968
- DOI: 10.3390/jcm8091327
Role of Bronchoscopic Techniques in the Diagnosis of Thoracic Sarcoidosis
Abstract
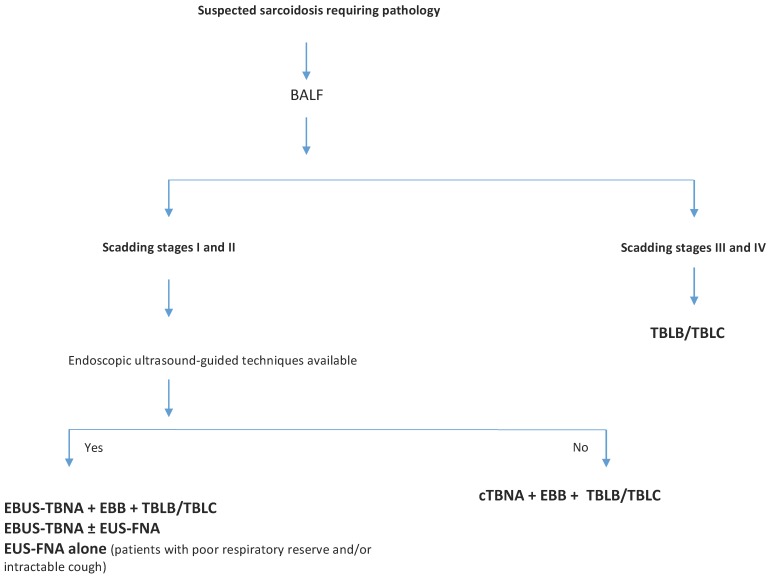
The diagnosis of sarcoidosis relies on clinical and radiological presentation, evidence of non-caseating granulomas in histopathology and exclusion of alternative causes of granulomatous inflammation. Currently, a proper diagnosis, with a high level of confidence, is considered as key to the appropriate diagnosis and management of the disease. In this sense, this review aims to provide a brief overview on the role of bronchoscopy in the diagnosis of thoracic sarcoidosis, incorporating newer techniques to establish, including endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA), endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA), transesophageal ultrasound-guided needle aspiration with the use of an echo bronchoscope (EUS-B-FNA) and transbronchial lung cryobiopsy (TBLC). Most of the literature reports the diagnostic superiority of endosonographic techniques, such as EBUS-TBNA alone or in combination with EUS-FNA, over conventional bronchoscopic modalities in diagnosing Scadding stages I and II of the disease. Moreover, TBLC may be considered a useful and safe diagnostic tool for thoracic sarcoidosis, overcoming some limitations of transbronchial lung biopsy (TBLB), avoiding more invasive modalities and being complementary to endosonographic procedures such as EBUS-TBNA.
Keywords: diagnosis; recent bronchoscopic techniques; sarcoidosis; standard bronchoscopic techniques.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hutchinson J. Anomalous Diseases of Skin and Fingers: Case of Livid Papillary psoriasis? Illus. Clin. Surg. 1877;1:42.
-
- ATS/ERS/WASOG Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ER. Am. J. Respir. Crit. Care Med. 1999;160:736–755. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
