

Proteus mirabilis endocarditis
- PMID: 31466989
- PMCID: PMC6721144
- DOI: 10.1136/bcr-2019-230575
Proteus mirabilis endocarditis
Abstract
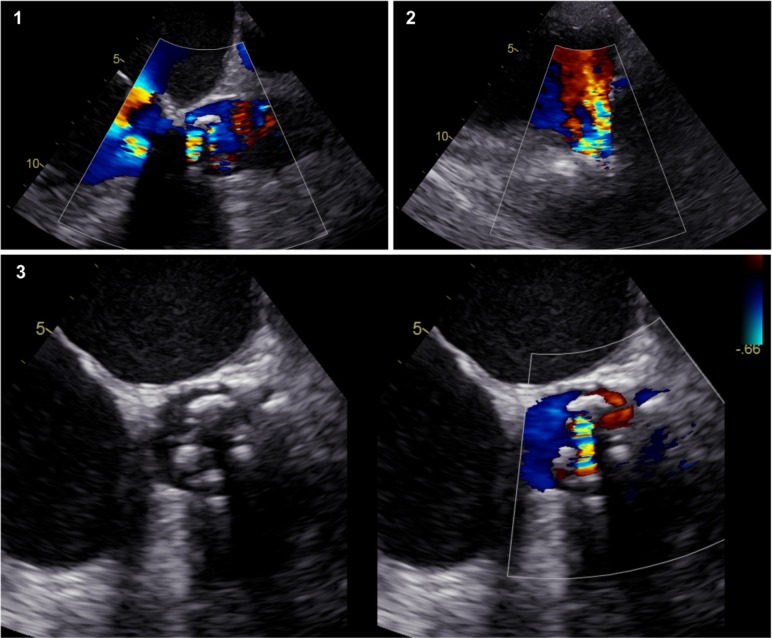
A 62-year-old man was admitted to the emergency department due to fever and acute heart failure. A transthoracic echocardiogram revealed severe aortic valve obstruction. He was an hepatic transplant recipient and was medicated with everolimus. He underwent mitral and aortic valve replacement with prosthetic valves 4 years ago. Due to his medical background, therapy and clinical presentation, empirical therapy for infective endocarditis was started. Transoesophageal echocardiogram showed severe aortic valve regurgitation but no other findings suggestive of endocarditis. Computed tomography (CT) revealed pulmonary infiltrates compatible with infection and no evidence of septic embolisation. Multiple sets of blood cultures were negative. Proteus mirabilis was isolated in bronchial lavage and antibiotic therapy was adjusted. The patient underwent aortic valve replacement, with no macroscopic findings suggestive of endocarditis. P. mirabilis was isolated in the surgically removed valve. Dual antibiotic therapy was successfully administered for 6 weeks.
Keywords: infections; valvar diseases.
© BMJ Publishing Group Limited 2019. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources