

Use of sodium glucose cotransporter 2 inhibitors and risk of major cardiovascular events and heart failure: Scandinavian register based cohort study
- PMID: 31467044
- PMCID: PMC6713906
- DOI: 10.1136/bmj.l4772
Use of sodium glucose cotransporter 2 inhibitors and risk of major cardiovascular events and heart failure: Scandinavian register based cohort study
Abstract
Objective: To investigate the cardiovascular effectiveness of sodium glucose cotransporter 2 (SGLT2) inhibitors in routine clinical practice.
Design: Cohort study using data from nationwide registers and an active-comparator new-user design.
Setting: Denmark, Norway, and Sweden, from April 2013 to December 2016.
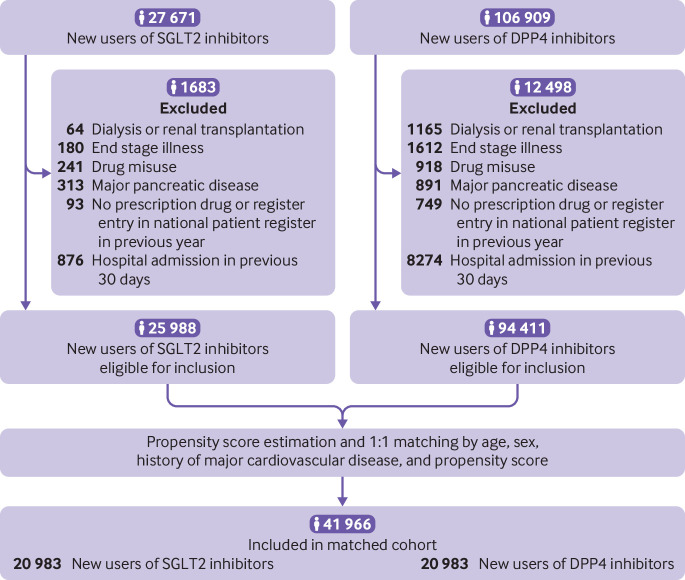
Participants: 20 983 new users of SGLT2 inhibitors and 20 983 new users of dipeptidyl peptidase 4 (DPP4) inhibitors, aged 35-84, matched by age, sex, history of major cardiovascular disease, and propensity score.
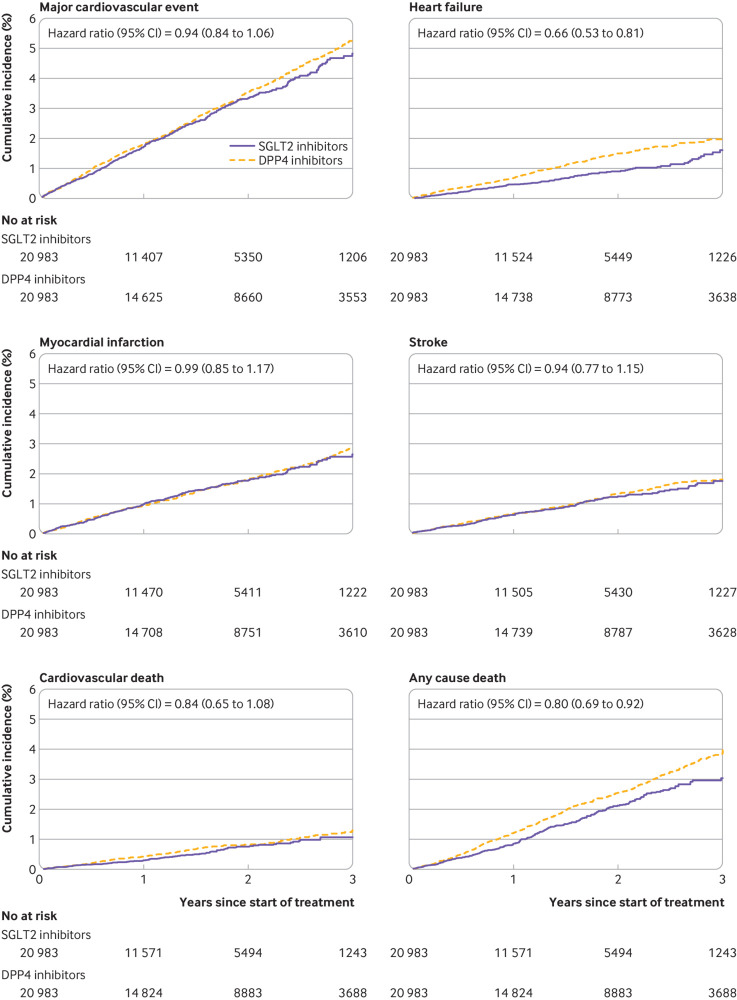
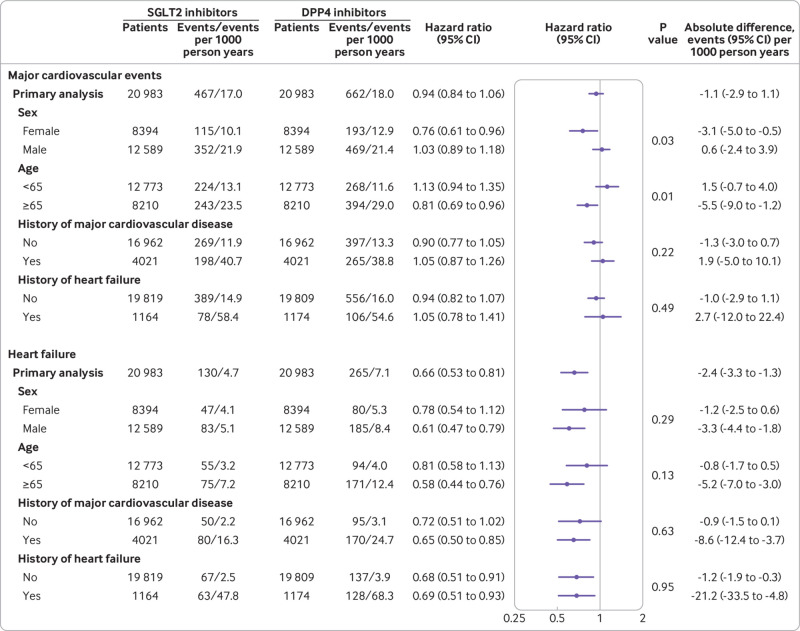
Main outcome measures: Primary outcomes were major cardiovascular events (composite of myocardial infarction, stroke, and cardiovascular death) and heart failure (hospital admission for heart failure or death due to heart failure). Secondary outcomes were the individual components of the cardiovascular composite and any cause death. In the primary analyses, patients were defined as exposed from treatment start throughout follow-up (analogous to intention to treat); additional analyses were conducted with an as-treated exposure definition. Cox regression was used to estimate hazard ratios.
Results: Mean age of the study cohort was 61 years, 60% were men, and 19% had a history of major cardiovascular disease. Of the total 27 416 person years of follow-up in the SGLT2 inhibitor group, 22 627 (83%) was among patients who initiated dapagliflozin, 4521 (16%) among those who initiated empagliflozin, and 268 (1%) among those who initiated canagliflozin. During follow-up, 467 SGLT2 inhibitor users (incidence rate 17.0 events per 1000 person years) and 662 DPP4 inhibitor users (18.0) had a major cardiovascular event, whereas 130 (4.7) and 265 (7.1) had a heart failure event, respectively. Hazard ratios were 0.94 (95% confidence interval 0.84 to 1.06) for major cardiovascular events and 0.66 (0.53 to 0.81) for heart failure. Hazard ratios were consistent among subgroups of patients with and without history of major cardiovascular disease and with and without history of heart failure. Hazard ratios for secondary outcomes, comparing SGLT2 inhibitors with DPP4 inhibitors, were 0.99 (0.85 to 1.17) for myocardial infarction, 0.94 (0.77 to 1.15) for stroke, 0.84 (0.65 to 1.08) for cardiovascular death, and 0.80 (0.69 to 0.92) for any cause death. In the as-treated analyses, hazard ratios were 0.84 (0.72 to 0.98) for major cardiovascular events, 0.55 (0.42 to 0.73) for heart failure, 0.93 (0.76 to 1.14) for myocardial infarction, 0.83 (0.64 to 1.07) for stroke, 0.67 (0.49 to 0.93) for cardiovascular death, and 0.75 (0.61 to 0.91) for any cause death.
Conclusions: In this large Scandinavian cohort, SGLT2 inhibitor use compared with DPP4 inhibitor use was associated with reduced risk of heart failure and any cause death, but not with major cardiovascular events in the primary intention-to-treat analysis. In the additional as-treated analyses, the magnitude of the association with heart failure and any cause death became larger, and a reduced risk of major cardiovascular events that was largely driven by the cardiovascular death component was observed. These data help inform patients, practitioners, and authorities regarding the cardiovascular effectiveness of SGLT2 inhibitors in routine clinical practice.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: support from the Swedish Heart-Lung Foundation, Novo Nordisk Foundation, and Swedish Society for Medical Research for the submitted work; BE has received personal fees for lectures and serving on advisory boards from Amgen, AstraZeneca, Boerhringer Ingelheim, Eli Lilly, Merck Sharp and Dohme, Mundipharma, Navamedic, Novo Nordisk, and RLS Global outside the submitted work, and research grants from Sanofi outside the submitted work; CJ has received personal fees for research consultancy work from Pfizer and Bayer outside of the submitted work; HS has received consulting fees from Celgene and is employed by IQVIA outside of the submitted work; SG has received lecture fees and research grants from AstraZeneca, Boerhringer Ingelheim, Eli Lilly, Merck Sharp and Dohme, Novo Nordisk, and Sanofi outside of the submitted work; the other authors did not have any potential competing interests to report.
Figures
References
-
- Kim YG, Han SJ, Kim DJ, Lee KW, Kim HJ. Association between sodium glucose co-transporter 2 inhibitors and a reduced risk of heart failure in patients with type 2 diabetes mellitus: a real-world nationwide population-based cohort study. Cardiovasc Diabetol 2018;17:91. 10.1186/s12933-018-0737-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous