

Enhancing Mesenchymal Stromal Cell Immunomodulation for Treating Conditions Influenced by the Immune System
- PMID: 31467564
- PMCID: PMC6701346
- DOI: 10.1155/2019/7219297
Enhancing Mesenchymal Stromal Cell Immunomodulation for Treating Conditions Influenced by the Immune System
Abstract
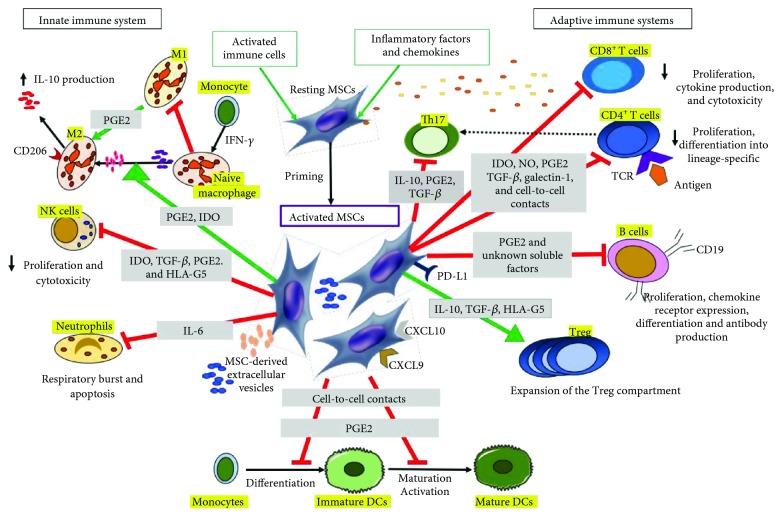
Mesenchymal stromal cells (MSCs), formerly known as mesenchymal stem cells, are nonhematopoietic multipotent cells and are emerging worldwide as the most clinically used and promising source for allogeneic cell therapy. MSCs, initially obtained from bone marrow, can be derived from several other tissues, such as adipose tissue, placenta, and umbilical cord. Diversity in tissue sourcing and manufacturing procedures has significant effects on MSC products. However, in 2006, a minimal set of standard criteria has been issued by the International Society of Cellular Therapy for defining derived MSCs. These include adherence to plastic in conventional culture conditions, particular phenotype, and multilineage differentiation capacity in vitro. Moreover, MSCs have trophic capabilities, a high in vitro self-renewal ability, and immunomodulatory characteristics. Thus, immunosuppressive treatment with MSCs has been proposed as a potential therapeutic alternative for conditions in which the immune system cells influence outcomes, such as inflammatory and autoimmune diseases. The precise mechanism by which MSCs affect functions of most immune effector cells is not completely understood but involves direct contact with immune cells, soluble mediators, and local microenvironmental factors. Recently, it has been shown that their homeostatic resting state requires activation, which can be achieved in vitro with various cytokines, including interferon-γ. In the present review, we focus on the suppressive effect that MSCs exert on the immune system and highlight the significance of in vitro preconditioning and its use in preclinical studies. We discuss the clinical aspects of using MSCs as an immunomodulatory treatment. Finally, we comment on the risk of interfering with the immune system in regard to cancer formation and development.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this paper.
Figures
References
-
- Ciuffreda M. C., Malpasso G., Musarò P., Turco V., Gnecchi M. Protocols for in vitro differentiation of human mesenchymal stem cells into osteogenic, chondrogenic and adipogenic lineages. In: Gnecchi M., editor. Mesenchymal Stem Cells. Vol. 1416. New York, NY, USA: Humana Press; 2016. pp. 149–158. (Methods in Molecular Biology). - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
