

Associations of Chronic Inflammation, Insulin Resistance, and Severe Obesity With Mortality, Myocardial Infarction, Cancer, and Chronic Pulmonary Disease
- PMID: 31469399
- PMCID: PMC6724168
- DOI: 10.1001/jamanetworkopen.2019.10456
Associations of Chronic Inflammation, Insulin Resistance, and Severe Obesity With Mortality, Myocardial Infarction, Cancer, and Chronic Pulmonary Disease
Abstract
Importance: Chronic inflammation and insulin resistance often accompany severe obesity, and all are associated with disease risk.
Objective: To examine how the association of severe obesity with adverse outcomes may be modified by the presence of systemic inflammation and/or insulin resistance.
Design, setting, and participants: This population-based, retrospective cohort study included all residents of Alberta, Canada, aged 18 years and older with at least 1 procedure to ascertain severe obesity and measures of C-reactive protein, fasting glucose, triglyceride, and high-density lipoprotein cholesterol levels. Participants were observed from April 2003 to March 2017, and data analysis was conducted from June 2018 to December 2018.
Exposures: Severe obesity (body mass index ≥35 or ≥40 after January 1, 2017, as indicated with a procedure-fee modifier), chronic inflammation (all measures of C-reactive protein >10 mg/L), and a surrogate measure of insulin resistance.
Main outcomes and measures: All-cause death, first acute myocardial infarction during follow-up, first cancer diagnosis during follow-up, and new chronic pulmonary disease.
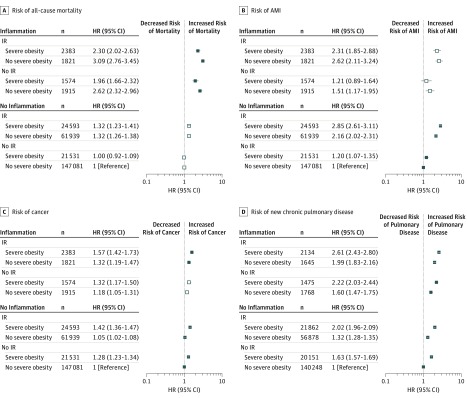
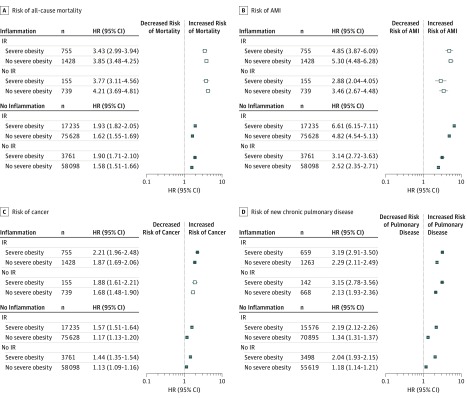
Results: Among 420 636 participants, the median age was 45 years (interquartile range, 34-56 years; range, 18-97 years), 157 799 (37.5%) were male, 185 782 (44.2%) had insulin resistance, 71 987 (17.1%) had severe obesity, and 10 770 (2.6%) had inflammation. In women with chronic inflammation, the presence of severe obesity was associated with a lower mortality risk (hazard ratio [HR], 0.75; 95% CI, 0.65-0.86), but there was no difference in risk in men with inflammation (HR, 0.89; 95% CI, 0.78-1.02). In contrast, the presence of severe obesity was associated with a higher mortality risk in men without inflammation (HR, 1.20; 95% CI, 1.13-1.26), but there was no difference in risk in women without inflammation (HR, 1.00; 95% CI, 0.95-1.06). For myocardial infarction, severe obesity was associated with increased risk in both women and men without inflammation (women: HR, 1.26; 95% CI, 1.17-1.36; men: HR, 1.35; 95% CI, 1.27-1.43) but not in women and men with inflammation (women: HR, 0.85; 95% CI, 0.67-1.07; men: HR, 0.90; 95% CI, 0.71-1.14). Severe obesity was associated with increased risk in women and men, irrespective of chronic inflammation, for new chronic pulmonary disease (women with inflammation: HR, 1.34; 95% CI, 1.23-1.46; women without inflammation: HR, 1.58; 95% CI, 1.54-1.62; men with inflammation: HR, 1.41; 95% CI, 1.29-1.54; men without inflammation: HR, 1.65; 95%, CI, 1.60-1.71) and cancer (women with inflammation: HR, 1.16; 95% CI, 1.03-1.30; women without inflammation, HR, 1.32; 95% CI, 1.28-1.36; men with inflammation: HR, 1.17; 95% CI, 1.04-1.32; men without inflammation: HR, 1.33; 95% CI, 1.28-1.39). Similar to chronic inflammation, severe obesity was not always associated with higher risk in participants with insulin resistance.
Conclusions and relevance: The findings suggest that severe obesity with systemic inflammation is associated with a different prognosis than severe obesity without inflammation.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
