

Cost-effectiveness analysis of reflex testing for Lynch syndrome in women with endometrial cancer in the UK setting
- PMID: 31469860
- PMCID: PMC6716649
- DOI: 10.1371/journal.pone.0221419
Cost-effectiveness analysis of reflex testing for Lynch syndrome in women with endometrial cancer in the UK setting
Abstract
Background: Lynch syndrome is a hereditary cancer syndrome caused by constitutional pathogenic variants in the DNA mismatch repair (MMR) system, leading to increased risk of colorectal, endometrial and other cancers. The study aimed to identify the incremental costs and consequences of strategies to identify Lynch syndrome in women with endometrial cancer.
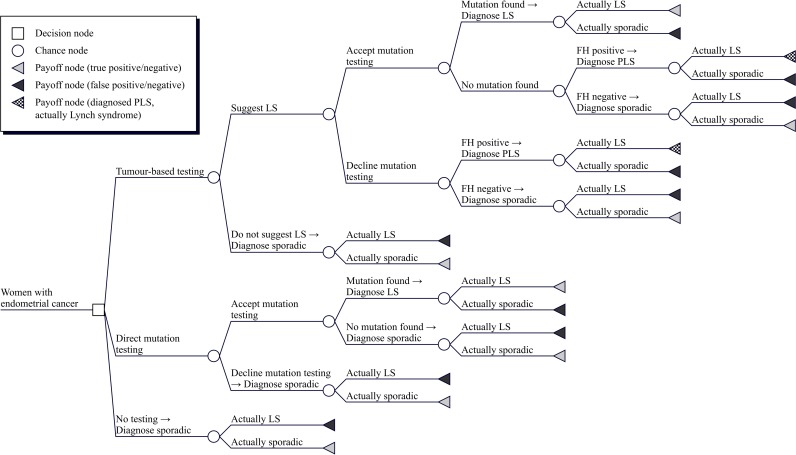
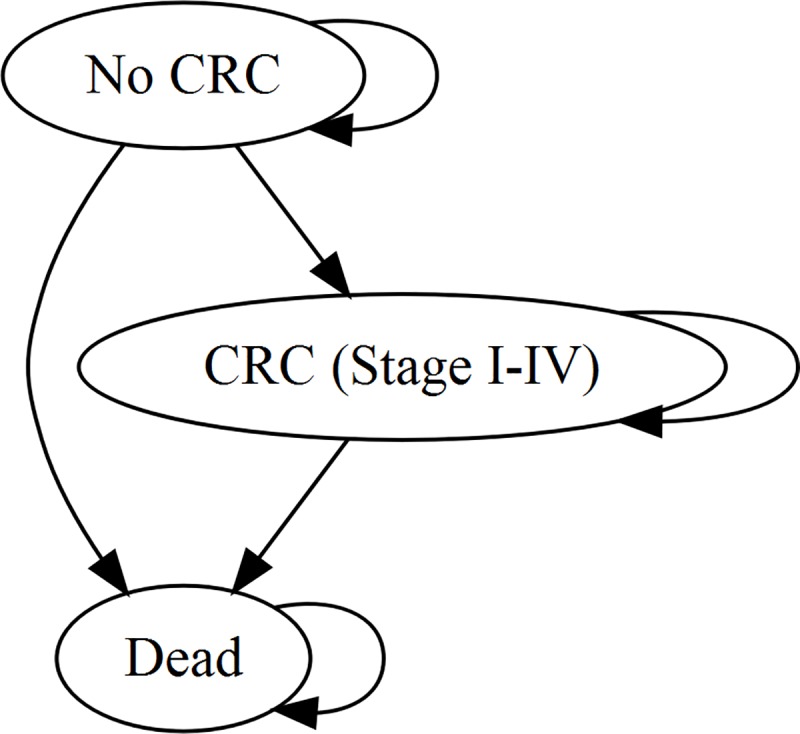
Methods: A decision-analytic model was developed to evaluate the relative cost-effectiveness of reflex testing strategies for identifying Lynch syndrome in women with endometrial cancer taking the NHS perspective and a lifetime horizon. Model input parameters were sourced from various published sources. Consequences were measured using quality-adjusted life years (QALYs). A cost-effectiveness threshold of £20 000/QALY was used.
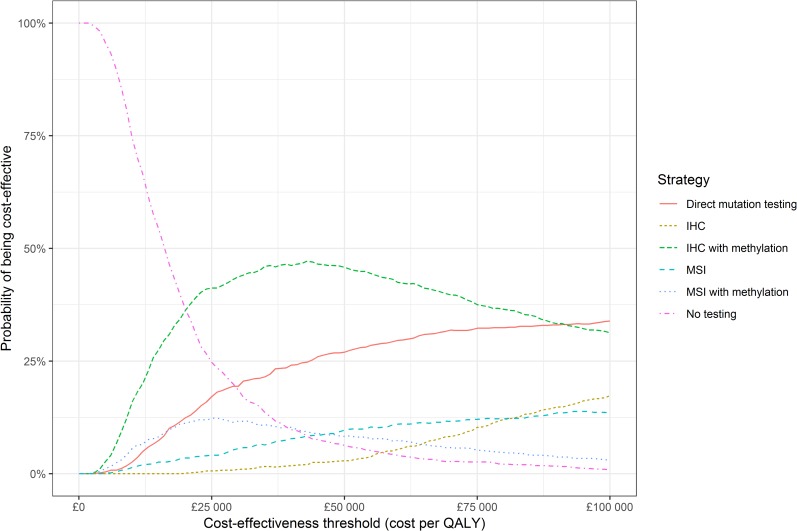
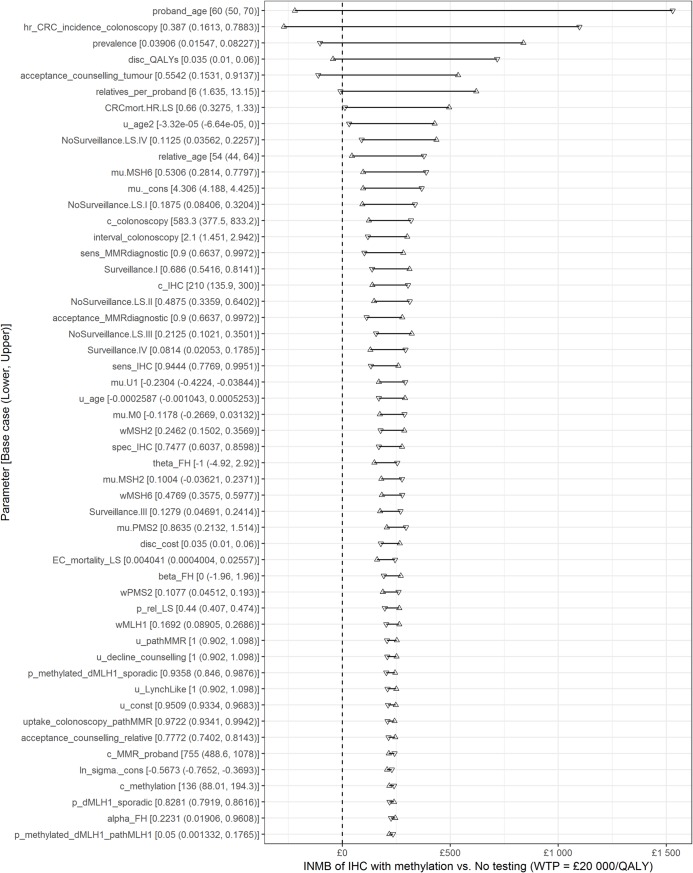
Results: Reflex testing for Lynch syndrome using MMR immunohistochemistry and MLH1 methylation testing was cost-effective versus no testing, costing £14 200 per QALY gained. There was uncertainty due to parameter imprecision, with an estimated 42% chance this strategy is not cost-effective compared with no testing. Age had a significant impact on cost-effectiveness, with testing not predicted to be cost-effective in patients aged 65 years and over.
Conclusions: Testing for Lynch syndrome in younger women with endometrial cancer using MMR immunohistochemistry and MLH1 methylation testing may be cost-effective. Age cut-offs may be controversial and adversely affect implementation.
Conflict of interest statement
IMF is an Honorary Medical Advisor to Lynch Syndrome UK and reports support from St Vincent’s University Hospital (Dublin), Impact Genetics (Bowmanville, Ontario, Canada), and Ambry Genetics (Aliso Viejo, CA, USA), for travel, outside the submitted work. Other authors declare no potential conflicts of interest. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
