

Two Years of Viral Metagenomics in a Tertiary Diagnostics Unit: Evaluation of the First 105 Cases
- PMID: 31470675
- PMCID: PMC6770117
- DOI: 10.3390/genes10090661
Two Years of Viral Metagenomics in a Tertiary Diagnostics Unit: Evaluation of the First 105 Cases
Abstract
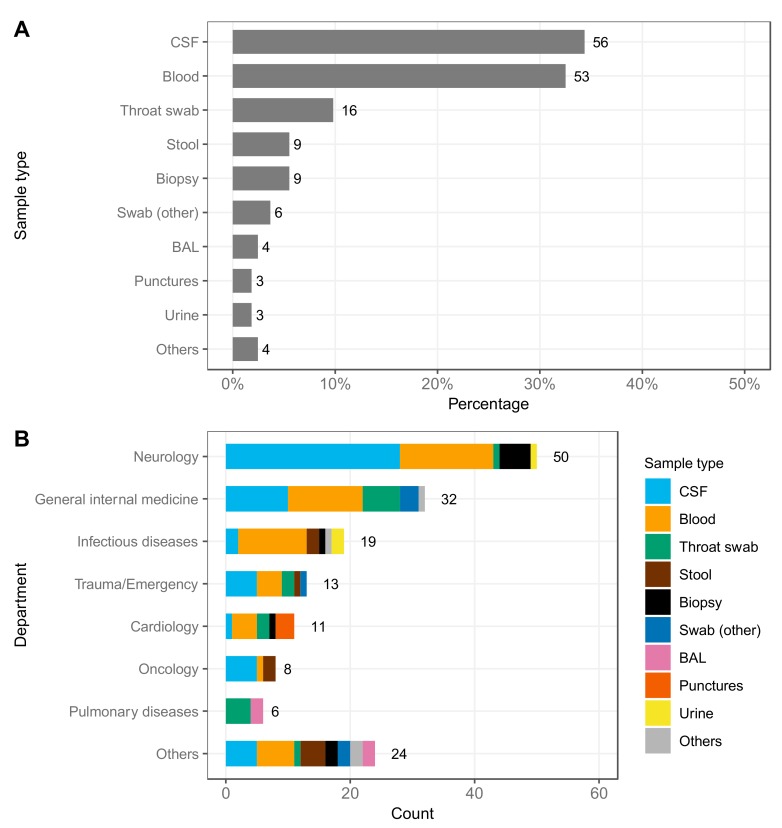
Metagenomic next-generation sequencing (mNGS) can capture the full spectrum of viral pathogens in a specimen and has the potential to become an all-in-one solution for virus diagnostics. To date, clinical application is still in an early phase and limitations remain. Here, we evaluated the impact of viral mNGS for cases analyzed over two years in a tertiary diagnostics unit. High throughput mNGS was performed upon request by the treating clinician in cases where the etiology of infection remained unknown or the initial differential diagnosis was very broad. The results were compared to conventional routine testing regarding outcome and workload. In total, 163 specimens from 105 patients were sequenced. The main sample types were cerebrospinal fluid (34%), blood (33%) and throat swabs (10%). In the majority of the cases, viral encephalitis/meningitis or respiratory infection was suspected. In parallel, conventional virus diagnostic tests were performed (mean 18.5 individually probed targets/patients). mNGS detected viruses in 34 cases (32%). While often confirmatory, in multiple cases, the identified viruses were not included in the selected routine diagnostic tests. Two years of mNGS in a tertiary diagnostics unit demonstrated the advantages of a single, untargeted approach for comprehensive, rapid and efficient virus diagnostics, confirming the utility of mNGS in complementing current routine tests.
Keywords: clinical impact; diagnostics; metagenomic sequencing; virus; virus infection.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Ewig S., Torres A., Angeles Marcos M., Angrill J., Rano A., de Roux A., Mensa J., Martinez J.A., de la Bellacasa J.P., Bauer T. Factors associated with unknown aetiology in patients with community-acquired pneumonia. Eur. Respir. J. 2002;20:1254–1262. doi: 10.1183/09031936.02.01942001. - DOI - PubMed
-
- Bleeker-Rovers C.P., Vos F.J., de Kleijn E.M., Mudde A.H., Dofferhoff T.S., Richter C., Smilde T.J., Krabbe P.F., Oyen W.J., van der Meer J.W. A prospective multicenter study on fever of unknown origin: The yield of a structured diagnostic protocol. Medicine (Baltimore) 2007;86:26–38. doi: 10.1097/MD.0b013e31802fe858. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
