

An augmented prescribed exercise program (APEP) to improve mobility of older acute medical patients - a randomized, controlled pilot and feasibility trial
- PMID: 31470815
- PMCID: PMC6716827
- DOI: 10.1186/s12877-019-1246-4
An augmented prescribed exercise program (APEP) to improve mobility of older acute medical patients - a randomized, controlled pilot and feasibility trial
Abstract
Background: There is inconclusive evidence for the effectiveness of additional exercise in older hospital patients. The aims of this study were (1) to assess the feasibility of an augmented prescribed exercise program (APEP) in older acute medical patients and (2) to measure the potential effects of APEP on mobility capacity in order to assess the feasibility of a large full-scale study.
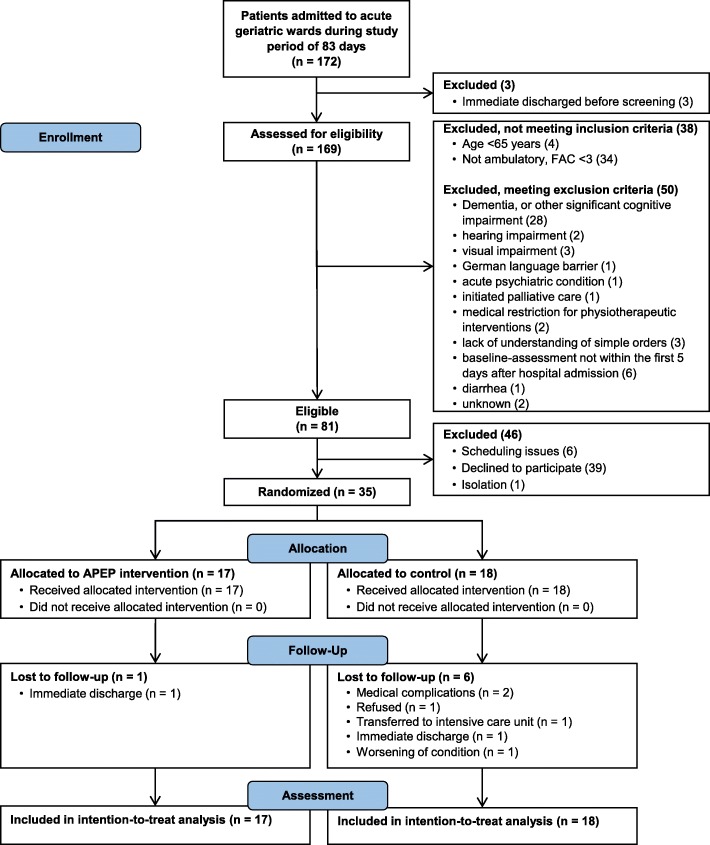
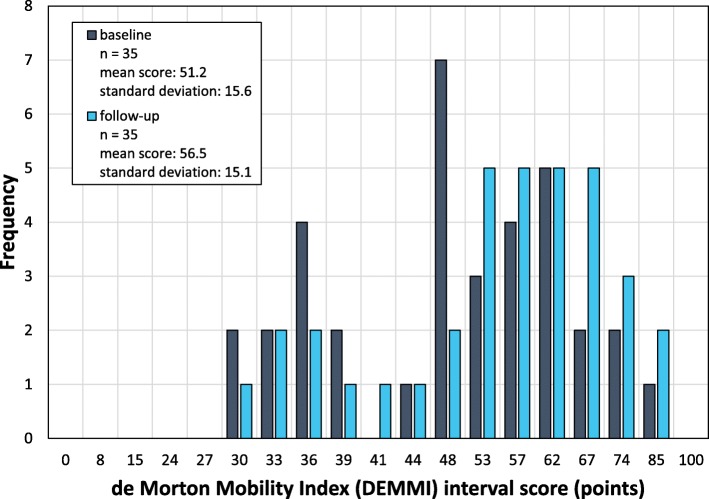
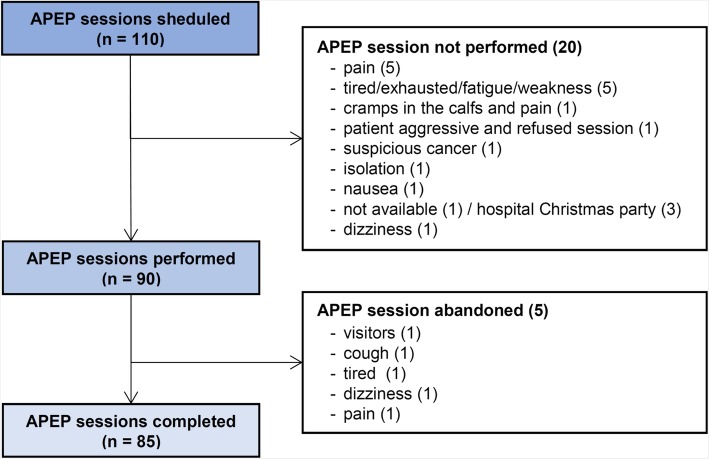
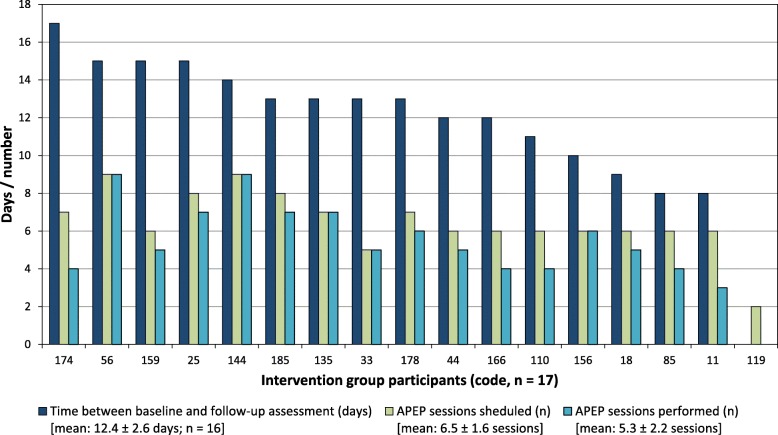
Methods: We conducted a single-center, prospective, parallel-group, single-blinded, randomized (1:1) controlled pilot and feasibility trial. Participants were recruited from acute geriatric wards of a general hospital. Key inclusion criteria were: age ≥ 65 years and walking ability. Key exclusion criteria were severe cognitive impairment and medical restriction for physical exercise interventions. Both groups received usual care, including physiotherapy. Intervention group participants were scheduled for additional exercise sessions (20-30 min, 4-5x/week). Feasibility of the trial design was assessed along pre-defined criteria for process, resources and management. Feasibility of the APEP intervention was analyzed by means of adherence, compliance and safety. Outcomes were measured at baseline and prior to hospital discharge. The primary outcome was mobility capacity (de Morton Mobility Index; DEMMI). Secondary outcomes were walking ability, physical endurance, fear of falling, frailty and length of stay.
Results: Thirty-five participants were recruited (recruitment rate 20.3%). We lost 7 participants to follow-up (retention rate: 80%). Intervention group participants (n = 17) each participated in 5.3 ± 2.2 additional exercise sessions (mean duration: 23.2 ± 4.0 min; mean adherence rate 78% ± 26%). No severe adverse events occurred during study assessments or APEP sessions. There were no statistically significant differences in mean change scores in any outcome measure. A sample of 124 participants would be required to detect a difference of 4 DEMMI points (ES = 0.45) with a power of 80%.
Conclusions: This small feasibility RCT indicates that an APEP intervention may be safe and feasible in older acute medical patients. APEP may possibly induce small to moderate effects on mobility, but the clinical relevance of these effects may be limited. These results inform the planning of a larger-scale phase III study.
Trial registration: German Clinical Trials Register ( DRKS00011262 ). Registered 27 October 2016.
Keywords: Exercise therapy; Hospitalization; Mobility limitation; Physiotherapy; Rehabilitation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
A study protocol of a randomised controlled trial to measure the effects of an augmented prescribed exercise programme (APEP) for frail older medical patients in the acute setting.BMC Geriatr. 2016 Apr 8;16:79. doi: 10.1186/s12877-016-0252-z. BMC Geriatr. 2016. PMID: 27059306 Free PMC article. Clinical Trial.
-
Enhancing physical activity in older adults receiving hospital based rehabilitation: a phase II feasibility study.BMC Geriatr. 2012 Jun 8;12:26. doi: 10.1186/1471-2318-12-26. BMC Geriatr. 2012. PMID: 22676723 Free PMC article. Clinical Trial.
-
Feasibility of trial procedures for a randomised controlled trial of a community based group exercise intervention for falls prevention for visually impaired older people: the VIOLET study.BMC Geriatr. 2018 Dec 12;18(1):307. doi: 10.1186/s12877-018-0998-6. BMC Geriatr. 2018. PMID: 30541483 Free PMC article. Clinical Trial.
-
Exercise Interventions Delivered Through Telehealth to Improve Physical Functioning for Older Adults with Frailty, Cognitive, or Mobility Disability: A Systematic Review and Meta-Analysis.Telemed J E Health. 2024 Apr;30(4):940-950. doi: 10.1089/tmj.2023.0177. Epub 2023 Nov 17. Telemed J E Health. 2024. PMID: 37975811 Free PMC article.
-
Non-pharmacological interventions targeting mobility among people with advanced cancer: a systematic review.Support Care Cancer. 2024 Aug 5;32(9):569. doi: 10.1007/s00520-024-08767-x. Support Care Cancer. 2024. PMID: 39102127 Free PMC article.
Cited by
-
Physiotherapy in acute geriatrics wards: What (de)motivates patients? A qualitative study based on self-determination theory.BMC Geriatr. 2024 Oct 23;24(1):866. doi: 10.1186/s12877-024-05474-4. BMC Geriatr. 2024. PMID: 39443854 Free PMC article.
-
Interrupting bedtime to reverse frailty levels in acute care: a study protocol for the Breaking Bad Rest randomized controlled trial.BMC Geriatr. 2023 Aug 10;23(1):482. doi: 10.1186/s12877-023-04172-x. BMC Geriatr. 2023. PMID: 37563553 Free PMC article.
-
Interventions to improve outdoor mobility among people living with disabilities: A systematic review.Campbell Syst Rev. 2024 Jun 14;20(2):e1407. doi: 10.1002/cl2.1407. eCollection 2024 Jun. Campbell Syst Rev. 2024. PMID: 38882933 Free PMC article. Review.
-
Frailty and Different Exercise Interventions to Improve Gait Speed in Older Adults after Acute Coronary Syndrome.Medicina (Kaunas). 2021 Dec 9;57(12):1344. doi: 10.3390/medicina57121344. Medicina (Kaunas). 2021. PMID: 34946289 Free PMC article. Clinical Trial.
-
The effects of nurse driven mobility intervention (NDMI) on activities of daily living, mobility, fear of falling, and balance performance in hospitalized older patients: A pilot study.Geriatr Nurs. 2023 Jan-Feb;49:193-198. doi: 10.1016/j.gerinurse.2022.12.006. Epub 2022 Dec 23. Geriatr Nurs. 2023. PMID: 36566605 Free PMC article.
References
-
- Callen BL, Mahoney JE, Wells TJ, Enloe M, Hughes S. Admission and discharge mobility of frail hospitalized older adults. Medsurg Nurs. 2004;13:156–163. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
