

Critical analysis and limitations of resting ankle-brachial index in the diagnosis of symptomatic peripheral arterial disease patients and the role of diabetes mellitus and chronic kidney disease
- PMID: 31471230
- PMCID: PMC7203622
- DOI: 10.1016/j.jvs.2019.05.050
Critical analysis and limitations of resting ankle-brachial index in the diagnosis of symptomatic peripheral arterial disease patients and the role of diabetes mellitus and chronic kidney disease
Abstract
Background: The ankle-brachial index (ABI) may underestimate the severity of peripheral arterial disease (PAD) in patients with noncompressible vessels. This study analyzed limitations of the ABI and toe-brachial index (TBI), if done alone, in patients with symptomatic PAD, diagnosed by duplex ultrasound (DUS) examination, particularly in patients with diabetes and chronic kidney disease (CKD).
Methods: This is a retrospective review of prospectively collected data. All patients underwent resting ABIs, TBI, and/or DUS. An ABIs of 0.90 or less in either leg was considered abnormal, and the term inconclusive ABIs (noncompressibility) was used if the ABI was 1.3 or greater. The sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy (OA) of ABIs in detecting 50% or greater stenosis of any arterial segment based on DUS were determined. A TBI of less than 0.7 was considered abnormal.
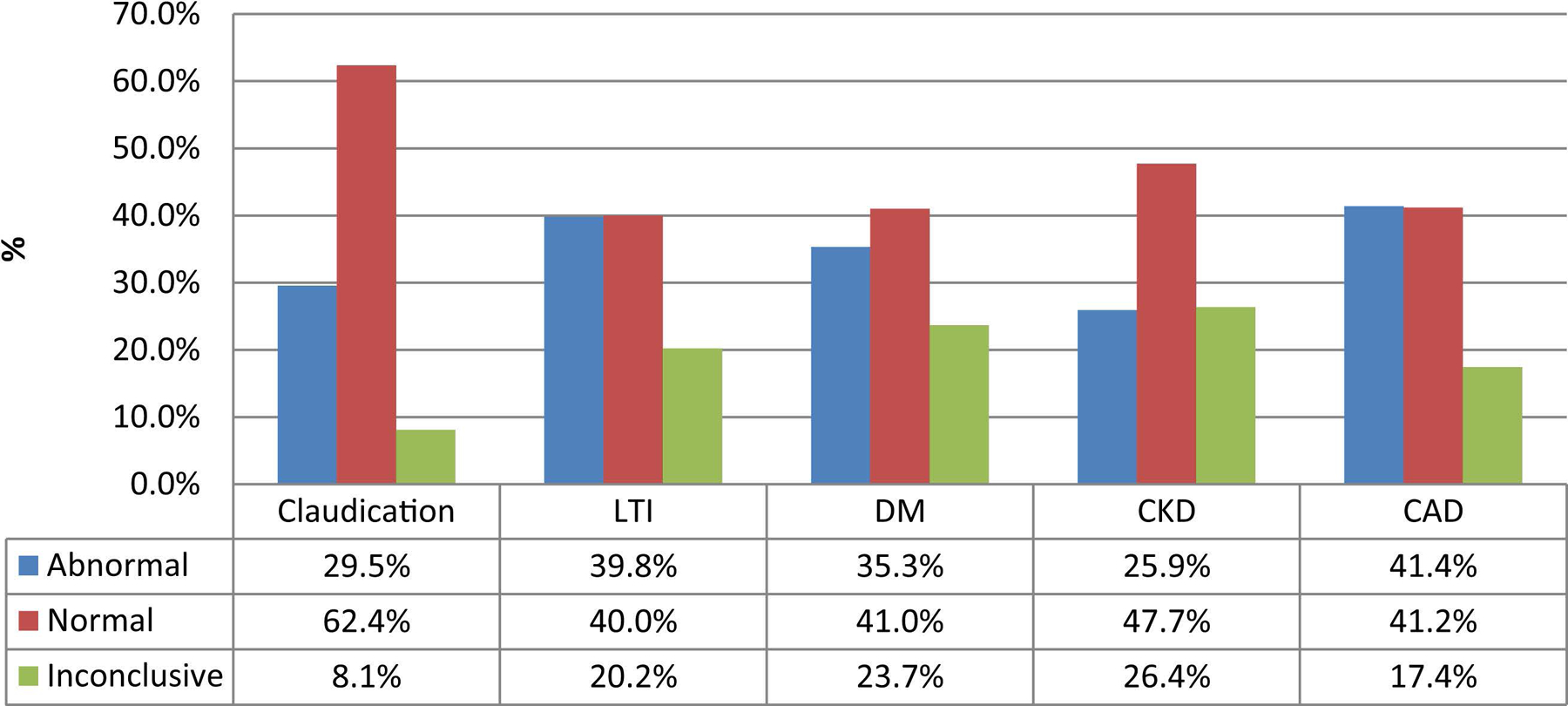
Results: We included 2226 ABIs and 1383 DUS examinations: 46% of patients had diabetes, 16% had CKD, and 39% had coronary artery disease. Fifty-three percent of the ABIs were normal, 34% were abnormal, and 13% were inconclusive. For patients with limb-threatening ischemia, 40% had normal ABIs, 40% abnormal ABIs, and 20% were inconclusive. The sensitivity and OA for ABIs in detecting 50% or greater stenosis in the whole series were 57% (95% confidence interval [CI], 53.7-61.2) and 74% (95% CI, 71.9-76.6); for diabetics 51% (95% CI, 46.1-56.3) and 66% (95% CI, 62.3-69.8); nondiabetics 66% (95% CI, 59.9-70.9) and 81% (95% CI, 78.2-83.9). For patients with CKD, the sensitivity and OA for ABIs in detecting 50% or greater stenosis was 43% (95% CI, 34.3-52.7) and 67% (95% CI, 60.2-73.0) versus patients with no CKD 60% (95% CI, 56.3-64.6) and 76% (95% CI, 73.1-78.1). If patients with inconclusive ABIs were excluded, these values were 69% (95% CI, 65.2-72.9) and 80% (95% CI, 77.2-81.9) in the whole series; 67% (95% CI, 61.6-72.7) and 75% (95% CI, 70.5-78.4) for diabetics; and 63% (95% CI, 51.3-73.0) and 78% (95% CI, 70.6-83.9) for patients with CKD. Thirty-three percent of TBIs were normal and 67% were abnormal. The sensitivity and OA for abnormal TBI in detecting 50% or greater stenosis were 85% (95% CI, 78.9-90.0) and 75% (95% CI, 70.1-80.2) in the whole series; 84% (95% CI, 76.0-90.3) and 74% (95% CI, 67.1-80.2) for diabetics; and 77% (95% CI, 61.4-88.2) and 72% (95% CI, 59.9-82.3) for patients with CKD. For those with inconclusive ABIs, these values for TBI were 75% and 69%.
Conclusions: Of symptomatic patients with PAD with 50% or greater stenosis on DUS examination, 43% had normal/inconclusive resting ABIs (49% in diabetics and 57% in CKD). TBI may help in patients with inconclusive ABIs. These patients should undergo further imaging to determine proper treatment.
Keywords: Ankle-brachial index; Chronic kidney disease; Diabetes mellitus; Peripheral arterial disease; Toe-brachial index.
Copyright © 2019 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author conflict of interest:
none.
Figures
References
-
- Kullo IH, Rooke TW. Peripheral arterial disease. N Engl J Med 2016;374:861–71. - PubMed
-
- Quigley FG, Faris IB, Duncan HJ. A comparison of Doppler ankle pressures and skin perfusion pressure in subjects with and without diabetes. Clin Physiol 1991;11:21–5. - PubMed
-
- Taguchi JT, Suwangool P. “Pipe-stem” brachial arteries: a cause of pseudohypertension. JAMA 1974;228:733. - PubMed
-
- Stein R, Hriljac I, Halperin JL, Gustavson SM, Teodorescu V, Olin JW. Limitation of the resting ankle-brachial index in symptomatic patients with peripheral arterial disease. Vasc Med 2006;11:29–33. - PubMed
-
- Koelemay MJ, den Hartog D, Prins MH, Kromhout JG, Legemate DA, Jacobs MJ. Diagnosis of arterial disease of the lower extremities with duplex ultrasonography. Br J Surg 1996;83:404–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
