

Dipeptidyl Peptidase 4 Inhibitors and Risk of Inflammatory Bowel Disease: Real-world Evidence in U.S. Adults
- PMID: 31471377
- PMCID: PMC6804610
- DOI: 10.2337/dc19-0162
Dipeptidyl Peptidase 4 Inhibitors and Risk of Inflammatory Bowel Disease: Real-world Evidence in U.S. Adults
Abstract
Objective: A recent study raises concerns that dipeptidyl peptidase 4 inhibitors (DPP4i) are associated with increased risk of inflammatory bowel disease (IBD). We evaluated the association between new use of DPP4i and IBD risk compared with other second-line antihyperglycemics.
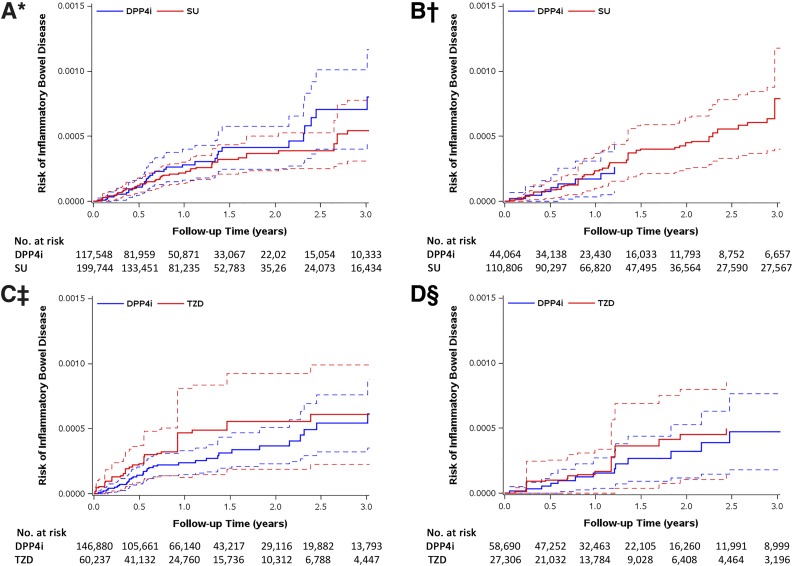
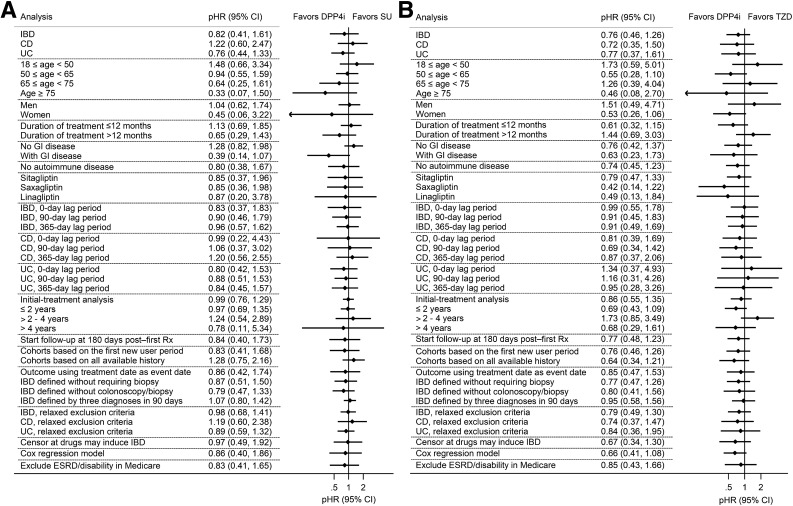
Research design and methods: We implemented an active-comparator, new-user cohort design using two U.S. administrative claims databases for commercially insured (MarketScan) and older adult (Medicare fee-for-service, 20% random sample) patients from January 2007 to December 2016. We identified patients, aged ≥18 years, who initiated DPP4i versus sulfonylureas (SUs) or initiated DPP4i versus thiazolidinediones (TZDs) and were without prior diagnosis, treatment, or procedure for IBD. The primary outcome was incident IBD, defined by IBD diagnosis preceded by colonoscopy and biopsy and followed by IBD treatment. We performed propensity score weighting to control for measured baseline confounding, estimated adjusted hazard ratios (aHRs [95% CI]) using weighted Cox proportional hazards models, and used random-effects meta-analysis models to pool aHRs across cohorts.
Results: We identified 895,747 eligible patients initiating DPP4i, SU, or TZD; IBD incidence rates ranged from 11.6 to 32.3/100,000 person-years. Over a median treatment duration of 1.09-1.69 years, DPP4i were not associated with increased IBD risk across comparisons. The pooled aHRs for IBD were 0.82 (95% CI 0.41-1.61) when comparing DPP4i (n = 161,612) to SU (n = 310,550) and 0.76 (0.46-1.26) when comparing DPP4i (n = 205,570) to TZD (n = 87,543).
Conclusions: Our population-based cohort study of U.S. adults with diabetes suggests that short-term DPP4i treatment does not increase IBD risk.
© 2019 by the American Diabetes Association.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
