

First pass effect with contact aspiration and stent retrievers in the Aspiration versus Stent Retriever (ASTER) trial
- PMID: 31471527
- PMCID: PMC7146919
- DOI: 10.1136/neurintsurg-2019-015215
First pass effect with contact aspiration and stent retrievers in the Aspiration versus Stent Retriever (ASTER) trial
Abstract
Background: The 'first pass effect' (FPE), which was originally described with stent retrievers, designates a (near-)complete revascularization obtained after a single device pass with no rescue therapy, and is associated with improved clinical outcome and decreased mortality.
Objective: We report the rate and benefits of FPE in the Aspiration versus Stent Retriever (ASTER) trial.
Materials and methods: ASTER is a randomized trial comparing angiographic revascularization with the stent retriever (SR) and contact aspiration (CA) thrombectomy techniques, assessed by an external core laboratory using the modified Thrombolysis in Cerebral Infarction (mTICI) scale. Rates of FPE (defined by mTICI 2c/3 after a single pass with no rescue therapy) were compared between patients treated with SR and CA techniques. Outcomes were compared between FPE-SR and FPE-CA patients, and between FPE and non-FPE patients.
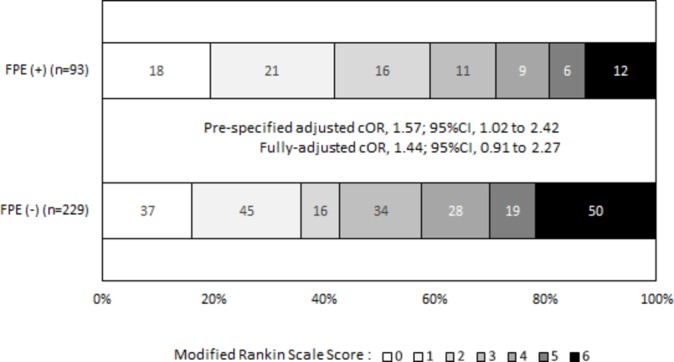
Results: FPE was achieved in 97/336 patients (28.9%), with no significant difference between SR and CA (respectively 53/169 patients (31.3%) vs 44/167 patients (26.3%), adjusted RR for CA versus SR 0.84, 95% CI 0.54 to 1.31; p=0.44). After prespecified adjustment for allocated arm and randomization stratification factors, FPE in patients was associated with a significantly improved clinical outcome and a decreased mortality, and a significantly lower rate of hemorrhagic transformation and procedural complications than in non-FPE patients.
Conclusion: In the ASTER trial, similar rates of FPE were achieved with SR and CA, and FPE was associated with a significantly improved outcome. New techniques and devices to improve the rate of FPE are warranted.
Trial registration number: Unique identifier: NCT02523261.
Keywords: recanalization; stroke; thrombectomy.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials