

Venous thromboembolism (VTE) prophylaxis in severely injured patients: an international comparative assessment
- PMID: 31471670
- PMCID: PMC7851035
- DOI: 10.1007/s00068-019-01208-z
Venous thromboembolism (VTE) prophylaxis in severely injured patients: an international comparative assessment
Abstract
Purpose: Venous thromboembolisms (VTE) are a major concern after acute survival from trauma. Variations in treatment protocols for trauma patients exist worldwide. This study analyzes the differences in the number of VTE events and the associated complications of thromboprophylaxis between two level I trauma populations utilizing varying treatment protocols.
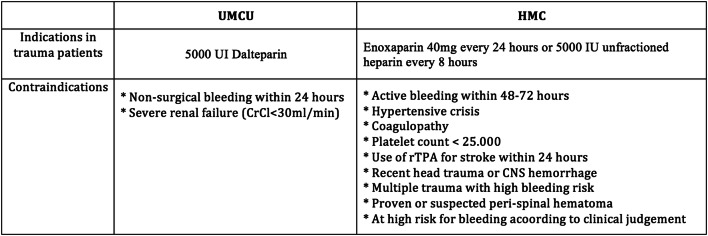
Methods: International multicenter trauma registry-based study was performed at the University Medical Center Utrecht (UMCU) in The Netherlands (early commencement chemical prophylaxis), and Harborview Medical Center (HMC) in the United States (restrictive early chemical prophylaxis). All severely injured patients (ISS ≥ 16), aged ≥ 18 years, and admitted in 2013 were included. Primary outcomes were VTE [deep venous thrombosis (DVT) (no screening), pulmonary embolism (PE)], and hemorrhagic complications.
Results: In UMCU, 279 patients were included and in HMC, 974 patients. Overall, 75% of the admitted trauma patients in UMCU and 81% in HMC (p < 0.001) received thromboprophylaxis, of which 100% in and 75% at, respectively, UMCU and HMC consisted of chemical prophylaxis. From these patients, 72% at UMCU and 47% at HMC (p < 0.001) were treated within 48 h after arrival. At UMCU, 4 patients (1.4%) (PE = 3, DVT = 1) and HMC 37 patients (3.8%) (PE = 22, DVT = 16; p = 0.06) developed a VTE. At UMCU, a greater percent of patients with VTE had traumatic brain injuries (TBI). Most VTE occurred despite adequate prophylaxis being given (75% UMCU and 81% HMC). Hemorrhagic complications occurred in, respectively, 4 (1.4%) and 10 (1%) patients in UMCU and HMC (p = 0.570). After adjustment for age, ISS, HLOS, and injury type, no significant difference was demonstrated in UMCU compared to HMC for the development of VTE, OR 2.397, p = 0.102 and hemorrhagic complications, OR 0. 586, p = 0.383.
Conclusions: A more early commencement protocol resulted in almost twice as much chemical prophylaxis being started within the first 48 h in comparison with a more delayed initiation of treatment. Interestingly, most episodes of VTE developed while receiving recommended prophylaxis. Early chemical thromboprophylaxis did not significantly increase the bleeding complications and it appears to be safe to start early.
Keywords: Bleeding complications; International comparative assessment; Severely injured patients; Thromboembolic events; Venous thromboembolism prophylaxis.
Conflict of interest statement
Amy Gunning received a grant from The Netherlands Organisation for Scientific Research to perform this research. Ronald Maier, Doret de Rooij, Luke Leenen, and Falco Hietbrink declare that they have no conflict of interest.
Figures
References
-
- World Health Organization. Injuries. 2014. https://www.who.int/topics/injuries/en/. Accessed 12 Mar 2015.
-
- Latronico N, Berardino M. Thromboembolic prophylaxis in head trauma and multiple-trauma patients. Minerva Anestesiol. 2008;74:543–548. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
