

Tumor mutational burden assessed by targeted NGS predicts clinical benefit from immune checkpoint inhibitors in non-small cell lung cancer
- PMID: 31471895
- PMCID: PMC6972587
- DOI: 10.1002/path.5344
Tumor mutational burden assessed by targeted NGS predicts clinical benefit from immune checkpoint inhibitors in non-small cell lung cancer
Abstract
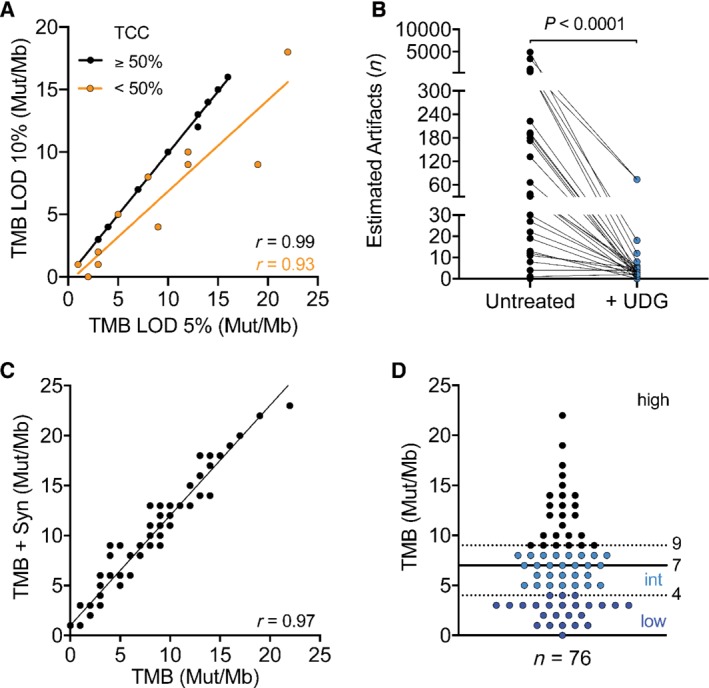
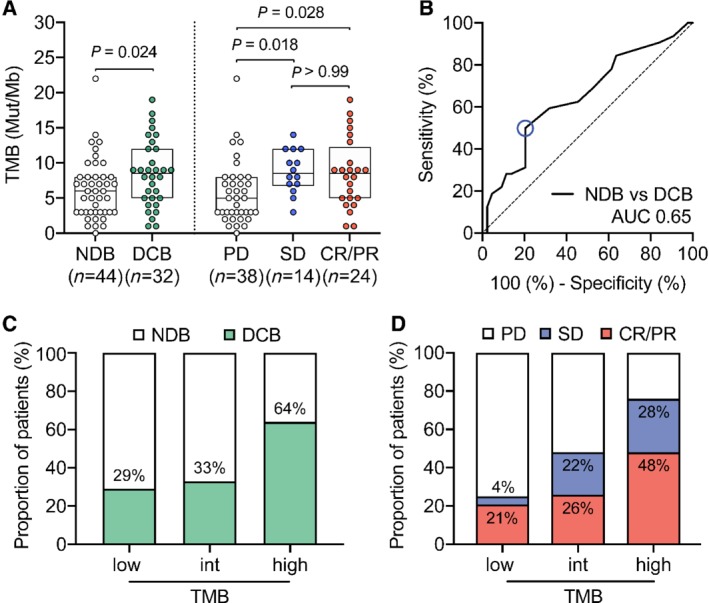
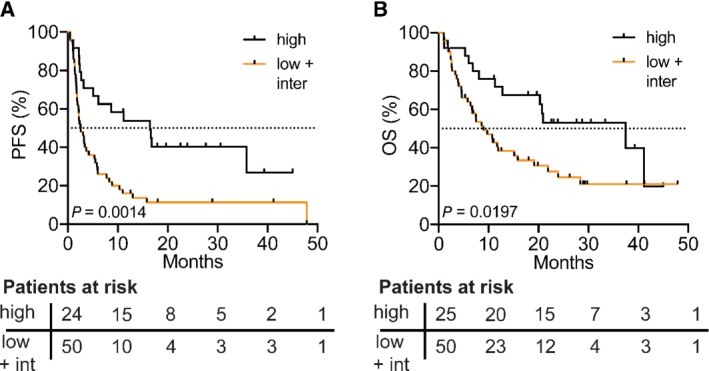
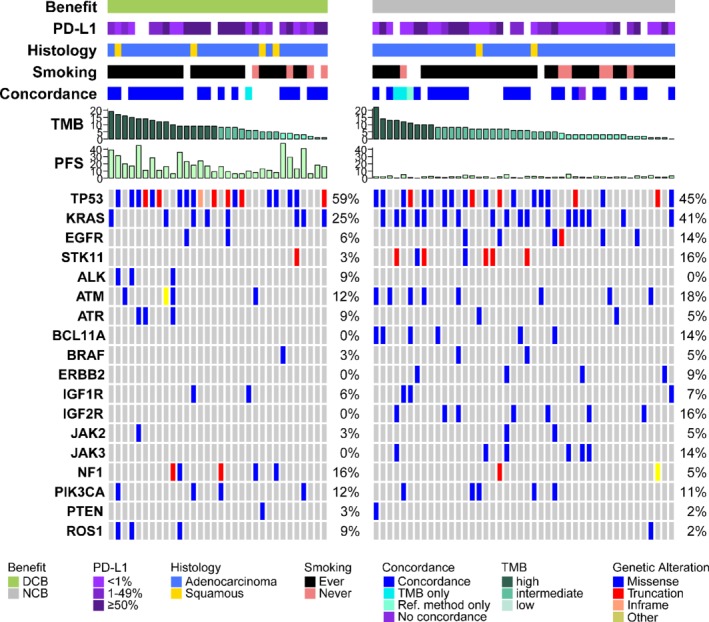
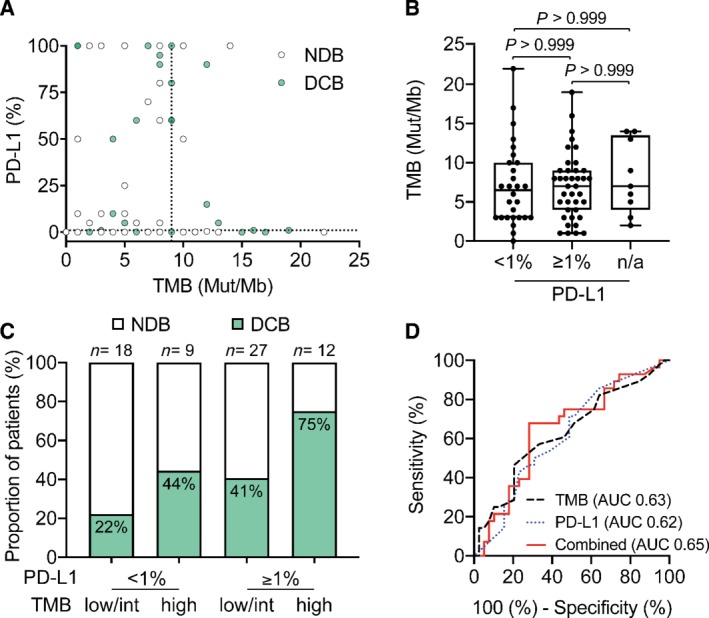
In non-small cell lung cancer (NSCLC), immune checkpoint inhibitors (ICIs) significantly improve overall survival (OS). Tumor mutational burden (TMB) has emerged as a predictive biomarker for patients treated with ICIs. Here, we evaluated the predictive power of TMB measured by the Oncomine™ Tumor Mutational Load targeted sequencing assay in 76 NSCLC patients treated with ICIs. TMB was assessed retrospectively in 76 NSCLC patients receiving ICI therapy. Clinical data (RECIST 1.1) were collected and patients were classified as having either durable clinical benefit (DCB) or no durable benefit (NDB). Additionally, genetic alterations and PD-L1 expression were assessed and compared with TMB and response rate. TMB was significantly higher in patients with DCB than in patients with NDB (median TMB = 8.5 versus 6.0 mutations/Mb, Mann-Whitney p = 0.0244). 64% of patients with high TMB (cut-off = third tertile, TMB ≥ 9) were responders (DCB) compared to 33% and 29% of patients with intermediate and low TMB, respectively (cut-off = second and first tertile, TMB = 5-9 and TMB ≤ 4, respectively). TMB-high patients showed significantly longer progression-free survival (PFS) and OS (log-rank test p = 0.0014 for PFS and 0.0197 for OS). While identifying different subgroups of patients, combining PD-L1 expression and TMB increased the predictive power (from AUC 0.63 to AUC 0.65). Our results show that the TML panel is an effective tool to stratify patients for ICI treatment. A combination of biomarkers might maximize the predictive precision for patient stratification. Our study supports TMB evaluation through targeted NGS in NSCLC patient samples as a tool to predict response to ICI therapy. We offer recommendations for a reliable and cost-effective assessment of TMB in a routine diagnostic setting. © 2019 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Keywords: NGS; NSCLC; TMB; cancer immunotherapy; checkpoint inhibitor.
© 2019 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Figures
References
-
- Reck M, Rodriguez‐Abreu D, Robinson AG, et al Pembrolizumab versus chemotherapy for PD‐L1‐positive non‐small‐cell lung cancer. N Engl J Med 2016; 375: 1823–1833. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
