

Effect of Sex, Age, and Positivity Threshold on Fecal Immunochemical Test Accuracy: A Systematic Review and Meta-analysis
- PMID: 31472152
- PMCID: PMC6878177
- DOI: 10.1053/j.gastro.2019.08.023
Effect of Sex, Age, and Positivity Threshold on Fecal Immunochemical Test Accuracy: A Systematic Review and Meta-analysis
Abstract
Background & aims: Quantitative fecal immunochemical tests (FITs) for hemoglobin are commonly used for colorectal cancer (CRC) screening. We aimed to quantify the change in CRC and advanced adenoma detection and number of positive test results at different positivity thresholds and by sex and age.
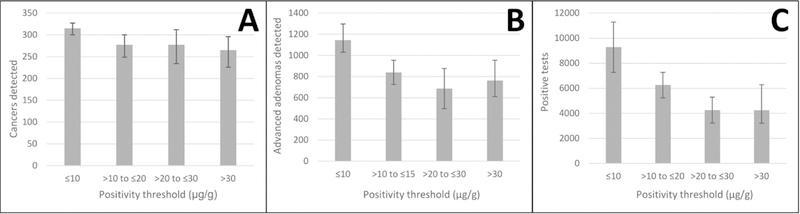
Methods: We searched MEDLINE and EMBASE, selecting articles of FIT for CRC detection in asymptomatic adults undergoing screening. We calculated sensitivity and specificity, as well as detected number of cancers, advanced adenomas, and positive test results at positivity thresholds ≤10 μg hemoglobin/g feces, 10 to ≤20 μg/g, 20 to ≤30 μg/g, and >30 μg/g. We also analyzed results from stratified by patient sex, age, and reference standard.
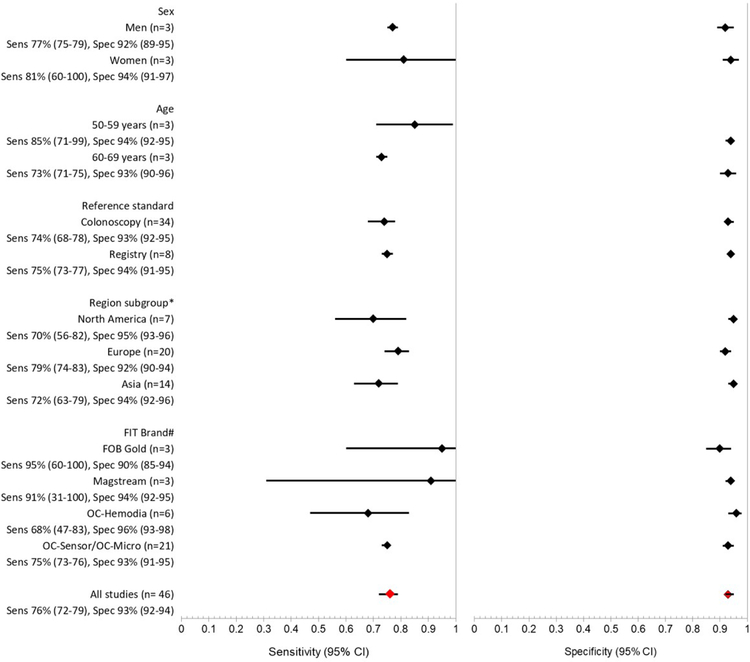
Results: Our meta-analysis comprised 46 studies with 2.4 million participants and 6478 detected cancers. Sensitivity for detection of CRC increased from 69% (95% confidence interval [CI], 63%-75%) at thresholds >10 μg/g and ≤20 μg/g to 80% (95% CI, 76%-83%) at thresholds ≤10 μg/g. At these threshold values, sensitivity for detection of advanced adenomas increased from 21% (95% CI, 18%-25%) to 31% (95% CI, 27%-35%), whereas specificity decreased from 94% (95% CI, 93%-96%) to 91% (95% CI, 89%-93%). In 3 studies stratified by sex, sensitivity of CRC detection was 77% in men (95% CI, 75%-79%) and 81% in women (95% CI, 60%-100%) (P = .68). In 3 studies stratified by age groups, sensitivity of CRC detection was 85% for ages 50-59 years (95% CI, 71%-99%) and 73% for ages 60-69 years (95% CI, 71%-75%) (P = .10). All studies with colonoscopy follow-up had similar sensitivity levels for detection of CRC to studies that analyzed 2-year registry follow-up data (74%; 95% CI, 68%-78% vs 75%; 95% CI, 73%-77%).
Conclusions: In a meta-analysis of studies that analyzed detection of CRC and advanced adenomas at different FIT positivity thresholds, we found the sensitivity and specificity of detection to vary with positive cutoff value. It might be possible to decrease positive threshold values for centers with sufficient follow-up colonoscopy resources. More research is needed to precisely establish FIT thresholds for each sex and age subgroup.
Protocol: PROSPERO CRD42017068760.
Keywords: Advanced Neoplasia; Colon Cancer; Diagnostic Performance; Fecal Occult Blood Test.
Copyright © 2019 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018;68:7–30. - PubMed
-
- Hewitson P, Glasziou P, Watson E, et al. Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (hemoccult): an update. Am J Gastroenterol 2008;103:1541–9. - PubMed
-
- Robertson DJ, Lee JK, Boland CR, et al. Recommendations on Fecal Immunochemical Testing to Screen for Colorectal Neoplasia: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2017;152:1217–1237 e3. - PubMed
-
- Force USPST, Bibbins-Domingo K, Grossman DC, et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2016;315:2564–75. - PubMed
-
- Vart G, Banzi R, Minozzi S. Comparing participation rates between immunochemical and guaiac faecal occult blood tests: a systematic review and meta-analysis. Prev Med 2012;55:87–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
