

Differential tractography as a track-based biomarker for neuronal injury
- PMID: 31472253
- PMCID: PMC6919327
- DOI: 10.1016/j.neuroimage.2019.116131
Differential tractography as a track-based biomarker for neuronal injury
Abstract
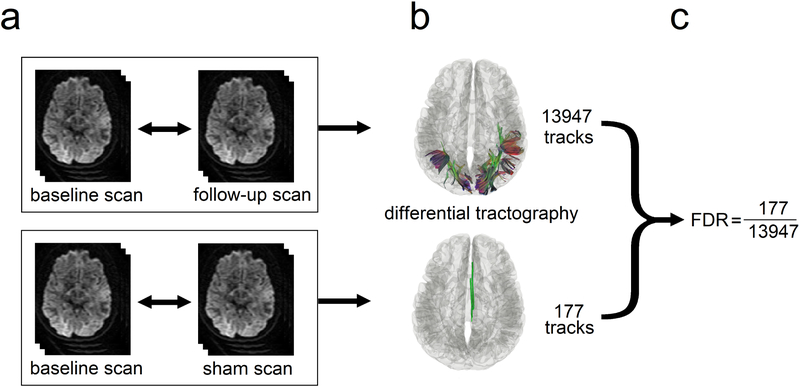
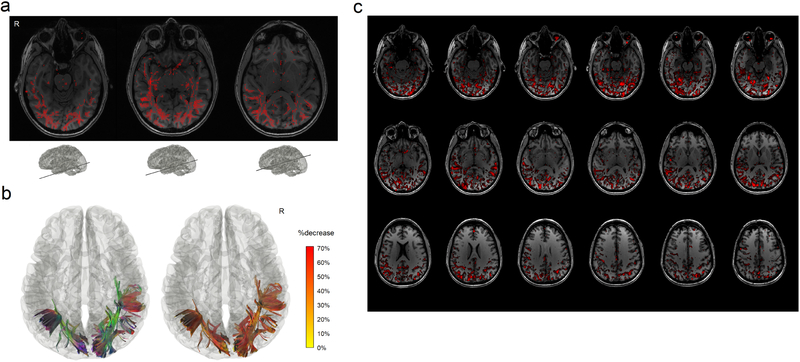
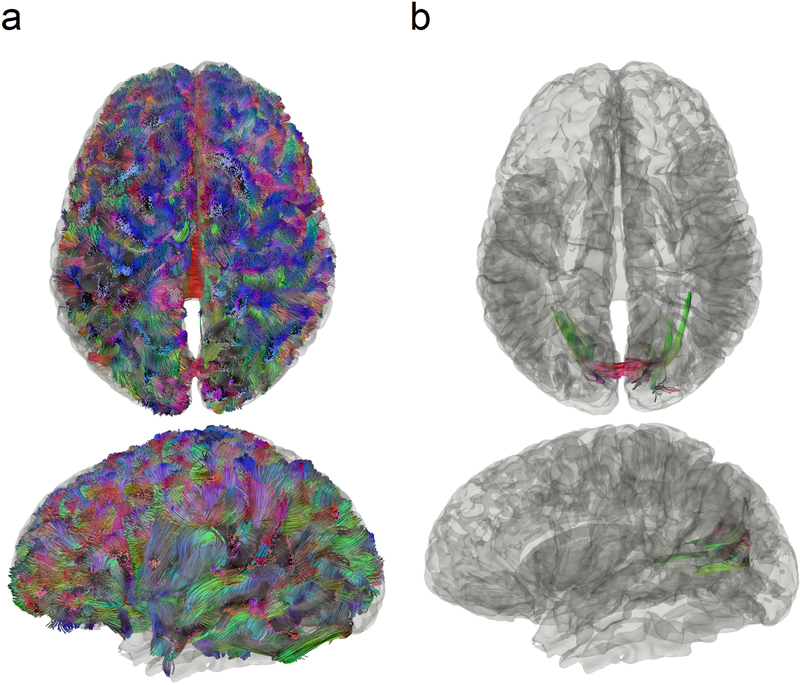
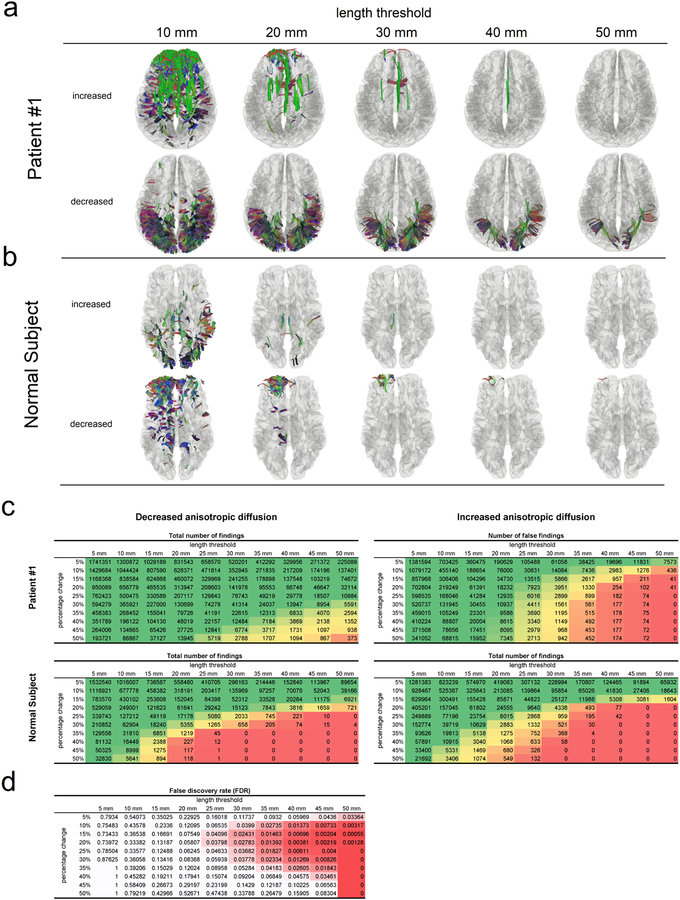
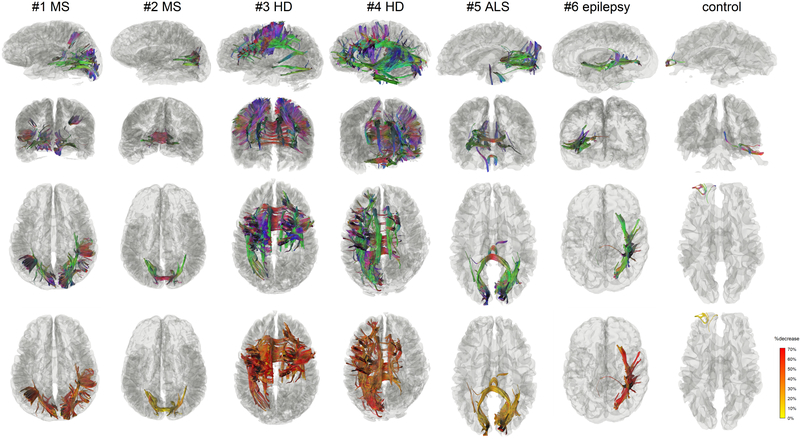
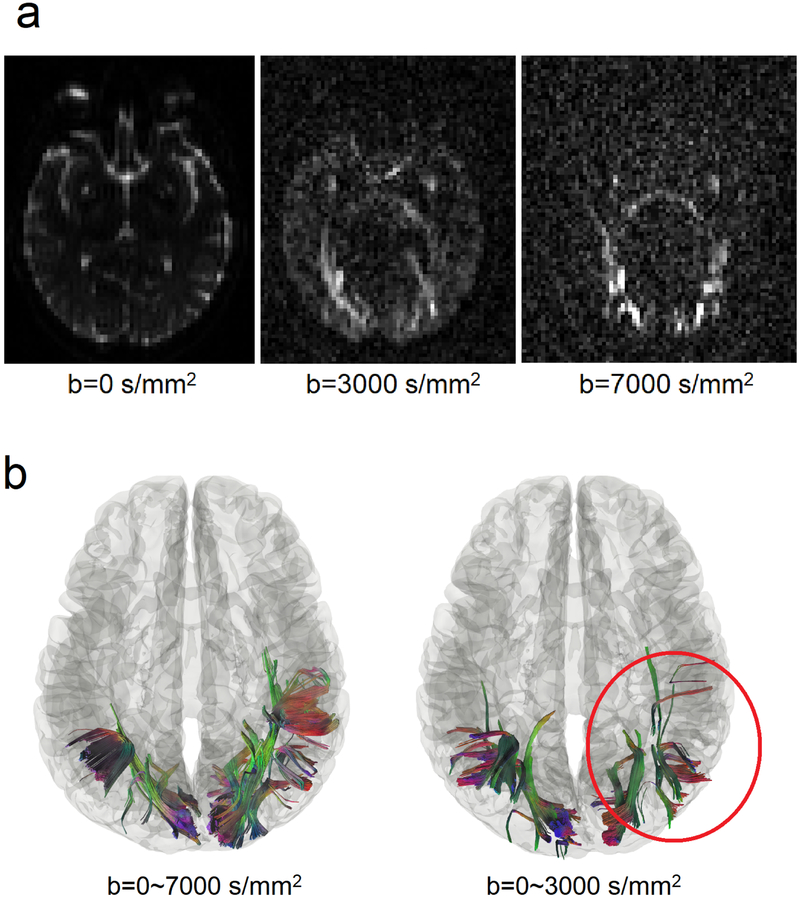
Diffusion MRI tractography has been used to map the axonal structure of the human brain, but its ability to detect neuronal injury is yet to be explored. Here we report differential tractography, a new type of tractography that utilizes repeat MRI scans and a novel tracking strategy to map the exact segment of fiber pathways with a neuronal injury. We examined differential tractography on multiple sclerosis, Huntington's disease, amyotrophic lateral sclerosis, and epileptic patients. The results showed that the affected pathways shown by differential tractography matched well with the unique clinical symptoms of the patients, and the false discovery rate of the findings could be estimated using a sham setting to provide a reliability measurement. This novel approach enables a quantitative and objective method to monitor neuronal injury in individuals, allowing for diagnostic and prognostic evaluation of brain diseases.
Keywords: Amyotrophic lateral sclerosis; Differential tractography; Diffusion MRI; Epilepsy; Fiber tracking; Huntington’s disease; Imaging biomarker; Multiple sclerosis; Neuronal injury.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures

References
-
- Ashburner J, Friston KJ, 2000. Voxel-based morphometry--the methods. Neuroimage 11, 805–821. - PubMed
-
- Basser PJ, Mattiello J, LeBihan D, 1994. Estimation of the effective self-diffusion tensor from the NMR spin echo. J Magn Reson B 103, 247–254. - PubMed
-
- Callaghan PT, 1991. Principles of Nuclear Magnetic Resonance Microscopy. Oxford University Press.
