

Dynamic quantitative nonenhanced magnetic resonance angiography of the abdominal aorta and lower extremities using cine fast interrupted steady-state in combination with arterial spin labeling: a feasibility study
- PMID: 31474219
- PMCID: PMC6717984
- DOI: 10.1186/s12968-019-0562-3
Dynamic quantitative nonenhanced magnetic resonance angiography of the abdominal aorta and lower extremities using cine fast interrupted steady-state in combination with arterial spin labeling: a feasibility study
Abstract
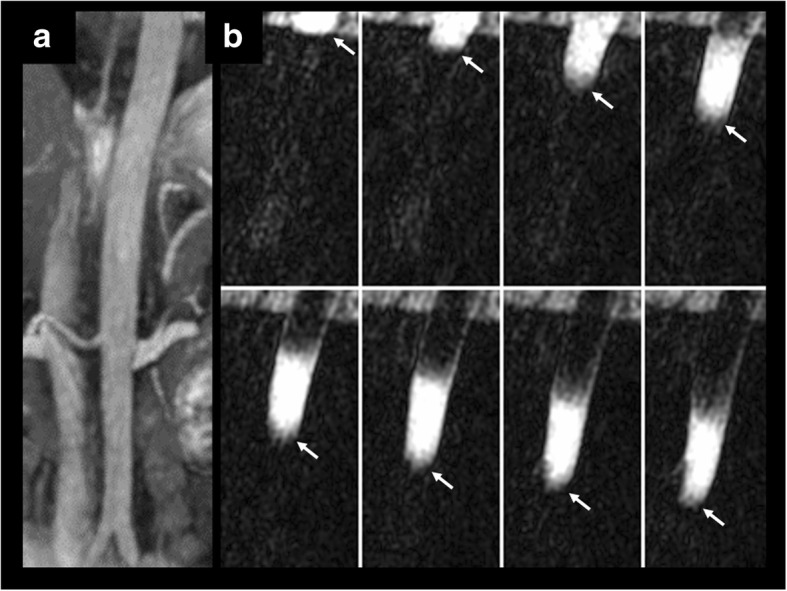
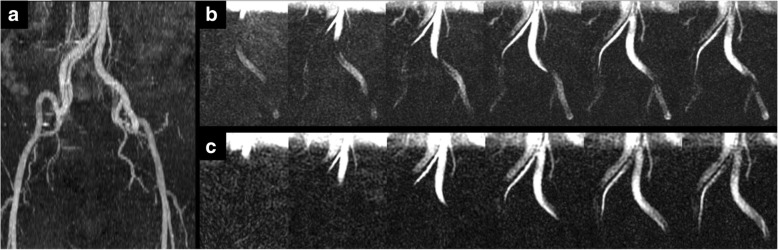
Background: Cine fast interrupted steady-state in combination with arterial spin labeling is a recently described nonenhanced magnetic resonance angiography (MRA) technique that relies on bolus tracking for time-resolved digital subtraction angiography-like displays of blood flow patterns. We evaluated the feasibility of applying this technique to display in-plane flow patterns in two regions: the abdominal aorta and lower extremity peripheral arteries.
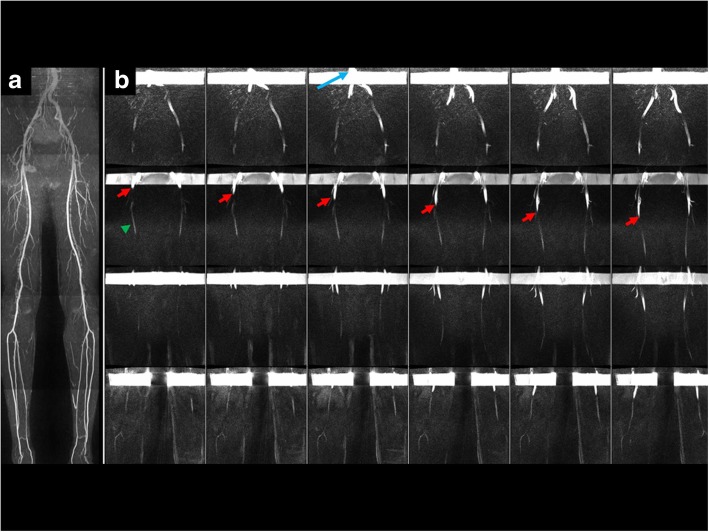
Methods: We performed an institutional review board-approved study in healthy subjects and patients. In 7 healthy subjects, in-plane flow was imaged at 4 stations ranging from the lower legs to the aorto-iliac bifurcation (junction of the distal thigh and upper calf, mid-thigh, junction of the upper thigh and pelvis, upper pelvis). In 5 healthy subjects and 6 patients without abdominal aortopathy, images were acquired through the suprarenal abdominal aorta. Ten patients with known peripheral arterial disease and two patients with stable disease of the abdominal aorta were also evaluated. Peak velocity was compared at each of the 4 stations for cine fast interrupted steady-state in combination with arterial spin labeling and two-dimensional cine phase contrast in patients with normal vessels.
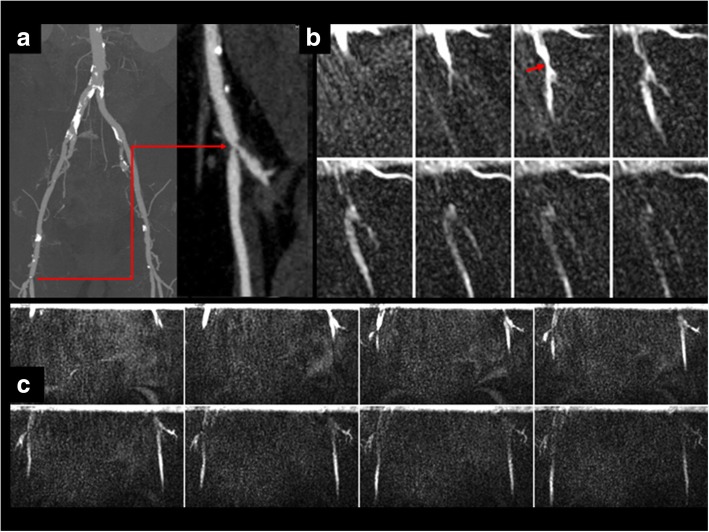
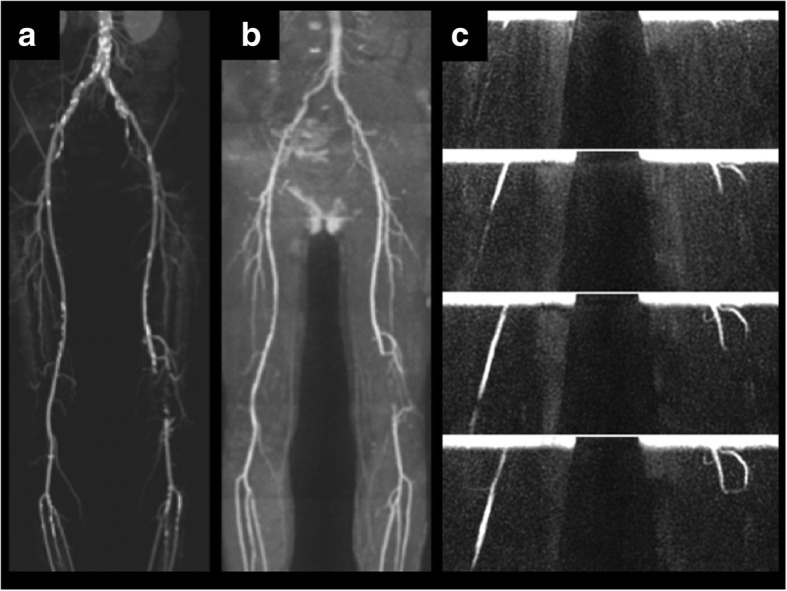
Results: In-plane flow patterns were well visualized in all peripheral arterial stations and in the abdominal aorta, providing a high quality display of hemodynamic patterns along extensive lengths of the vessels. There was very strong positive correlation (r = 0.952, P < 0.05) and excellent agreement (intraclass correlation coefficient, 0.935; 95% confidence interval, 0.812-0.972) between peak flow velocities measured by cine fast interrupted steady-state in combination with arterial spin labeling and two-dimensional cine phase contrast. In 10 patients with peripheral artery disease and 2 patients with aortic pathology, cine fast interrupted steady-state in combination with arterial spin labeling provided a visual demonstration of abnormal hemodynamics.
Conclusion: This feasibility study suggests that cine fast interrupted steady-state in combination with arterial spin labeling provides an efficient, high quality and physiologically accurate display of in-plane flow patterns over extensive lengths of the lower extremity peripheral arteries, which can be difficult to achieve using other MRA techniques.
Keywords: Angiography; Fast interrupted steady-state; Flow measurement; Magnetic resonance imaging; Peripheral artery disease; Quiescent interval slice-selective.
Conflict of interest statement
EAA: None
IK: Research support from Siemens Healthcare
BBL: None
RRE: Research support and royalty arrangement with Siemens Healthcare
Figures



Similar articles
-
Cardiovascular cine imaging and flow evaluation using Fast Interrupted Steady-State (FISS) magnetic resonance.J Cardiovasc Magn Reson. 2018 Feb 19;20(1):12. doi: 10.1186/s12968-018-0433-3. J Cardiovasc Magn Reson. 2018. PMID: 29458384 Free PMC article.
-
Accuracy of Noncontrast Quiescent-Interval Single-Shot Lower Extremity MR Angiography Versus CT Angiography for Diagnosis of Peripheral Artery Disease: Comparison With Digital Subtraction Angiography.JACC Cardiovasc Imaging. 2017 Oct;10(10 Pt A):1116-1124. doi: 10.1016/j.jcmg.2016.09.030. Epub 2017 Jan 18. JACC Cardiovasc Imaging. 2017. PMID: 28109932
-
Fast MR angiography of the aortoiliac arteries and arteries of the lower extremity: value of bolus-enhanced, whole-volume subtraction technique.AJR Am J Roentgenol. 1995 Aug;165(2):431-7. doi: 10.2214/ajr.165.2.7618572. AJR Am J Roentgenol. 1995. PMID: 7618572
-
Noncontrast Magnetic Resonance Angiography for the Diagnosis of Peripheral Vascular Disease.Circ Cardiovasc Imaging. 2019 May;12(5):e008844. doi: 10.1161/CIRCIMAGING.118.008844. Circ Cardiovasc Imaging. 2019. PMID: 31088154 Review.
-
Noncontrast MR angiography: An update.J Magn Reson Imaging. 2019 Feb;49(2):355-373. doi: 10.1002/jmri.26288. Epub 2018 Dec 19. J Magn Reson Imaging. 2019. PMID: 30566270 Free PMC article. Review.
Cited by
-
Background suppression single-shot electrocardiogram trigger non-enhanced magnetic resonance angiography in lower extremity blood vessels: a comparative study.Quant Imaging Med Surg. 2025 Feb 1;15(2):1312-1323. doi: 10.21037/qims-24-1120. Epub 2025 Jan 22. Quant Imaging Med Surg. 2025. PMID: 39995725 Free PMC article.
-
Quantification of Iliac Arterial Blood Velocity in Stenotic Phantom and Porcine Models Using Quantitative Digital Subtraction Angiography.J Vasc Interv Radiol. 2024 Sep;35(9):1357-1366. doi: 10.1016/j.jvir.2023.12.013. Epub 2023 Dec 21. J Vasc Interv Radiol. 2024. PMID: 38141780 Free PMC article.
References
-
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. - DOI - PMC - PubMed
-
- Gerhard-Herman MD, Gornik HL, Barrett C, Barshes NR, Corriere MA, Drachman DE, et al. 2016 AHA/ACC guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2017;69(11):e71–e126. doi: 10.1016/j.jacc.2016.11.007. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
