

Safety and clinical outcomes of endoscopic ultrasound-guided gallbladder drainage with lumen-apposing metal stents in patients with dwell time over one year
- PMID: 31474799
- PMCID: PMC6686095
- DOI: 10.20524/aog.2019.0395
Safety and clinical outcomes of endoscopic ultrasound-guided gallbladder drainage with lumen-apposing metal stents in patients with dwell time over one year
Abstract
Background: Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) has proved effective in patients with cholecystitis at high surgical risk. The long-term risks of gallstone-related disease and stent-related adverse events are unknown.
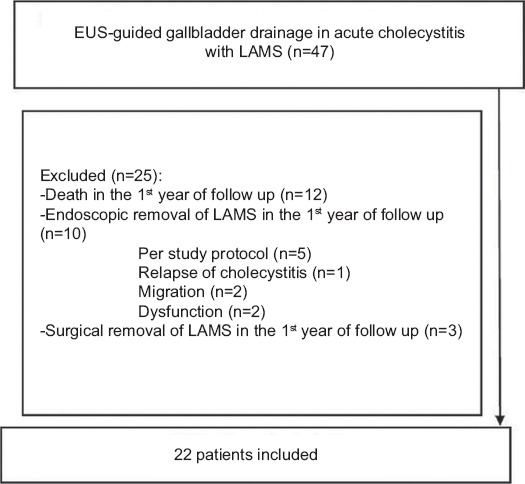
Methods: We performed a retrospective evaluation of a case series including subjects who underwent EUS-GBD using lumen-apposing metal stents (LAMS). Patients were identified from a prospective LAMS registry at a single tertiary center. Patients with a stent indwell time <1 year were excluded. Data regarding stent deployment and adverse events were retrieved from the prospective LAMS registry, while emergency room visits, admissions and causes of death were retrieved from electronic medical records.
Results: We included 22 patients with a median age of 88.3 years (interquartile range [IQR]: 82.6-92.7), 14 (63.6%) were male. Median follow up was 24.4 months (IQR: 18.2-42.4) and median time to the last available imaging procedure was 607 days (IQR: 463-938). No LAMS-related adverse events were identified beyond the first year of follow up. During follow up, 12 patients (54.5%) visited the emergency room 34 times (1 visit/patient, IQR: 0-3) and a total of 36 hospital admissions were required, with a median of 1 admission/patient (IQR: 0-3). Fourteen (63.6%) patients died during follow up. Only 1 patient (4.5%) required new hospital admissions for gallstone-related disease.
Conclusions: There were no adverse events beyond the first year after stent deployment, with only 4.5% of subjects requiring gallstone-related admissions. Permanent EUS-GBD with LAMS may be a definitive treatment for acute cholecystitis in patients ineligible for cholecystectomy.
Keywords: Cholecystitis; digestive system; drainage; endoscopy; stents.
Conflict of interest statement
Conflict of Interest: Raúl Torres Yuste, Javier García-Alonso, Ramón Sánchez-Ocana Hernández, Marta Cimavilla Román, Irene Peñas Herrero, Ana Yaiza Carbajo, Marina De Benito Sanz and Carlos De la Serna Higuera have no conflicts of interest or financial ties to disclose; Manuel Pérez-Miranda: Consultant: GI tech, Boston-Scientific, Gore. Speaker: Boston-Scientific, Olympus
Figures
Similar articles
-
Endoscopic ultrasound-guided gallbladder drainage with long-term lumen-apposing metal stent indwell: 1-year results from a prospective nationwide observational study.J Gastroenterol Hepatol. 2024 Feb;39(2):360-368. doi: 10.1111/jgh.16392. Epub 2023 Nov 3. J Gastroenterol Hepatol. 2024. PMID: 37920889
-
Comparison of the effectiveness and safety of lumen-apposing metal stents and anti-migrating tubular self-expandable metal stents for EUS-guided gallbladder drainage in high surgical risk patients with acute cholecystitis.Gastrointest Endosc. 2020 Mar;91(3):543-550. doi: 10.1016/j.gie.2019.09.042. Epub 2019 Oct 17. Gastrointest Endosc. 2020. PMID: 31629721
-
Similar Efficacies of Endoscopic Ultrasound Gallbladder Drainage With a Lumen-Apposing Metal Stent Versus Percutaneous Transhepatic Gallbladder Drainage for Acute Cholecystitis.Clin Gastroenterol Hepatol. 2017 May;15(5):738-745. doi: 10.1016/j.cgh.2016.12.021. Epub 2016 Dec 30. Clin Gastroenterol Hepatol. 2017. PMID: 28043931
-
EUS guided gallbladder drainage.Transl Gastroenterol Hepatol. 2020 Jul 5;5:41. doi: 10.21037/tgh.2019.12.20. eCollection 2020. Transl Gastroenterol Hepatol. 2020. PMID: 32632392 Free PMC article. Review.
-
Efficacy and Safety of Lumen Apposing Self-Expandable Metal Stents for EUS Guided Cholecystostomy: A Meta-Analysis and Systematic Review.Can J Gastroenterol Hepatol. 2018 Apr 12;2018:7070961. doi: 10.1155/2018/7070961. eCollection 2018. Can J Gastroenterol Hepatol. 2018. PMID: 29850458 Free PMC article.
Cited by
-
Endoscopic Gallbladder Drainage: A Comprehensive Review on Indications, Techniques, and Future Perspectives.Medicina (Kaunas). 2024 Apr 14;60(4):633. doi: 10.3390/medicina60040633. Medicina (Kaunas). 2024. PMID: 38674279 Free PMC article. Review.
-
How to perform EUS-guided biliary drainage.Endosc Ultrasound. 2022 Sep-Oct;11(5):342-354. doi: 10.4103/EUS-D-21-00188. Endosc Ultrasound. 2022. PMID: 36255022 Free PMC article. Review.
-
Endoscopic Ultrasound-Guided Gallbladder Drainage: Current Perspectives.Clin Exp Gastroenterol. 2020 May 15;13:193-201. doi: 10.2147/CEG.S203626. eCollection 2020. Clin Exp Gastroenterol. 2020. PMID: 32523368 Free PMC article. Review.
-
Endoscopic Management of Gallbladder Disease.Curr Gastroenterol Rep. 2023 Oct;25(10):250-254. doi: 10.1007/s11894-023-00886-5. Epub 2023 Nov 2. Curr Gastroenterol Rep. 2023. PMID: 37914915 Review.
-
Endoscopic transpapillary gallbladder stenting vs percutaneous cholecystostomy for managing acute cholecystitis: Nationwide propensity score study.Endosc Int Open. 2025 Feb 26;13:a25210084. doi: 10.1055/a-2521-0084. eCollection 2025. Endosc Int Open. 2025. PMID: 40018071 Free PMC article.
References
-
- Yamashita Y, Takada T, Strasberg SM, et al. Tokyo Guideline Revision Committee. TG13 surgical management of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2013;20:89–96. - PubMed
-
- Tsuyuguchi T, Itoi T, Takada T, et al. Tokyo Guideline Revision Committee. TG13 indications and techniques for gallbladder drainage in acute cholecystitis (with videos) J Hepatobiliary Pancreat Sci. 2013;20:81–88. - PubMed
-
- García-Alonso FJ, de Lucas Gallego, Bonillo Cambrodón D, et al. Gallstone-related disease in the elderly:is there room for improvement? Dig Dis Sci. 2015;60:1770–1777. - PubMed
-
- Choi JH, Lee SS, Choi JH, et al. Long-term outcomes after endoscopic ultrasonography-guided gallbladder drainage for acute cholecystitis. Endoscopy. 2014;46:656–661. - PubMed
-
- Baron TH, Grimm IS, Swanstrom LL. Interventional approaches to gallbladder disease. N Engl J Med. 2015;373:357–365. - PubMed
LinkOut - more resources
Full Text Sources