

History of Hypertension Is Associated With MR Hypoperfusion in Chinese Inpatients With DWI-Negative TIA
- PMID: 31474927
- PMCID: PMC6702658
- DOI: 10.3389/fneur.2019.00867
History of Hypertension Is Associated With MR Hypoperfusion in Chinese Inpatients With DWI-Negative TIA
Abstract
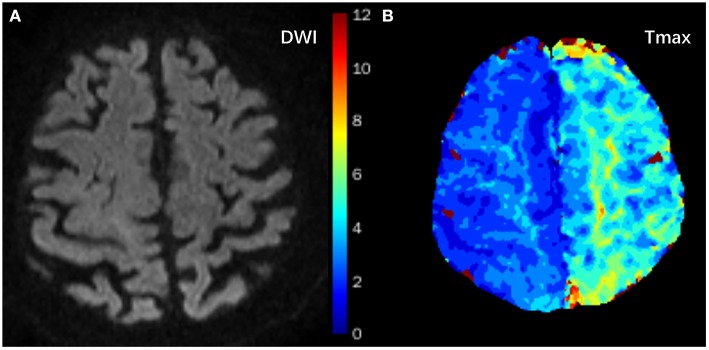
Objectives: The present study aimed to examine the prevalence of and risk factors for magnetic resonance (MR) perfusion abnormality in a Chinese population with transient ischemic attack (TIA) and normal diffusion-weighted imaging (DWI) findings. Methods: Patients with TIA admitted to our stroke center between January 2015 and October 2017 were recruited to the present study. MRI, including both DWI and perfusion-weighted imaging (PWI), was performed within 7 days of symptom onset. Time to maximum of the residue function (Tmax) maps were evaluated using the RAPID software (Ischemaview USA, Version 4.9) to determine hypoperfusion. Multivariate analysis was used to assess perfusion findings, clinical variables, medical history, cardio-metabolic, and the ABCD2 scores (age, blood pressure, clinical features, symptom duration, and diabetes). Results: Fifty-nine patients met the inclusion criteria. The prevalence of MR perfusion Tmax ≥ 4 s ≥ 0 ml and ≥ 10 mL were 72.9% (43/59) and 42.4% (25/59), respectively. Multivariate analyses revealed that history of hypertension is an independent factor associated with MR perfusion abnormality (Tmax ≥ 4 s ≥ 10 mL) for Chinese patients with TIA (P = 0.033, adjusted OR = 4.11, 95% CI = 1.12-15.11). Proximal artery stenosis (>50%) tended to lead to a larger PW lesion on MRI (p = 0.067, adjusted OR = 3.60, 95% CI = 0.91-14.20). Conclusion: Our results suggest that the prevalence of perfusion abnormality is high as assessed by RAPID using the parametric Tmax ≥ 4 s. History of hypertension is a strong predictor of focal perfusion abnormality as calculated by RAPID on Tmax map of TIA patients with negative DWI findings.
Keywords: DWI; PWI; hypertension; risk factors; transient ischemic attack.
Figures
Similar articles
-
Risk factors of perfusion and diffusion abnormalities on MRI in hemispheric TIA: a case-control study.Ann Transl Med. 2019 Dec;7(24):808. doi: 10.21037/atm.2019.12.69. Ann Transl Med. 2019. PMID: 32042824 Free PMC article.
-
Tissue-Negative Transient Ischemic Attack: Is There a Role for Perfusion MRI?AJR Am J Roentgenol. 2016 Jul;207(1):157-62. doi: 10.2214/AJR.15.15447. Epub 2016 Apr 12. AJR Am J Roentgenol. 2016. PMID: 27070836
-
Yield of combined perfusion and diffusion MR imaging in hemispheric TIA.Neurology. 2009 Mar 31;72(13):1127-33. doi: 10.1212/01.wnl.0000340983.00152.69. Epub 2008 Dec 17. Neurology. 2009. PMID: 19092109 Free PMC article.
-
Role of Perfusion-Weighted Imaging in a Diffusion-Weighted-Imaging-Negative Transient Ischemic Attack.J Clin Neurol. 2017 Apr;13(2):129-137. doi: 10.3988/jcn.2017.13.2.129. Epub 2017 Jan 12. J Clin Neurol. 2017. PMID: 28176500 Free PMC article.
-
Risk Factors of Hypoperfusion on MRI of Ischemic Stroke Patients Within 7 Days of Onset.Front Neurol. 2021 May 7;12:668360. doi: 10.3389/fneur.2021.668360. eCollection 2021. Front Neurol. 2021. PMID: 34025571 Free PMC article.
Cited by
-
Multimodal MRI study of the relationship between plaque characteristics and hypoperfusion in patients with transient ischemic attack.Front Neurol. 2023 Sep 28;14:1242923. doi: 10.3389/fneur.2023.1242923. eCollection 2023. Front Neurol. 2023. PMID: 37840913 Free PMC article.
-
Power of Hypoperfusion in Predicting Recurrent Transient Ischemic Attacks: Protocol of a Prospective Cohort Study.Front Hum Neurosci. 2021 Jun 24;15:654383. doi: 10.3389/fnhum.2021.654383. eCollection 2021. Front Hum Neurosci. 2021. PMID: 34248522 Free PMC article.
-
Emergency Presentations for Dizziness-Radiological Findings, Final Diagnoses, and Mortality.Int J Clin Pract. 2023 Jun 20;2023:7450009. doi: 10.1155/2023/7450009. eCollection 2023. Int J Clin Pract. 2023. PMID: 37383705 Free PMC article.
-
The Frequency and Associated Factors of Asymmetrical Prominent Veins: A Predictor of Unfavorable Outcomes in Patients with Acute Ischemic Stroke.Neural Plast. 2021 Sep 17;2021:9733926. doi: 10.1155/2021/9733926. eCollection 2021. Neural Plast. 2021. PMID: 34567108 Free PMC article.
-
Vasculo-Neuronal Coupling and Neurovascular Coupling at the Neurovascular Unit: Impact of Hypertension.Front Physiol. 2020 Sep 25;11:584135. doi: 10.3389/fphys.2020.584135. eCollection 2020. Front Physiol. 2020. PMID: 33101063 Free PMC article. Review.
References
-
- Easton JD, Saver JL, Albers GW, Alberts MJ, Chaturvedi S, Feldmann E, et al. . Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. (2009) 40:2276–93. 10.1161/STROKEAHA.108.192218 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous